5 min Show recovery of the patient after fluid treatment
advertisement

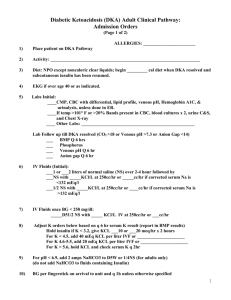
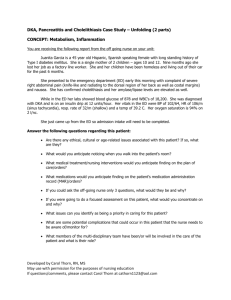
Appendix B Full handout given to participants SIMULATION OF DKA FOR CMBMP Cellular and Molecular Basics of Medical Practice January 29 - February 2, 2007 Facilitators’ Guide for DKA Simulation “Tiffany: The Soccer Player” Simulation Development and Cognitive Science Laboratory DEPARTMENT OF MEDICAL EDUCATION FACULTY: Developers: Department of Anesthesiology, Department of Physiology: Instructors: Technical Assistance: Help with Original Development: Learning Objectives: overall: Based on the lecture material and upon completion of the simulation, students should be able to: 1. Describe the major causative factors of diabetic ketoacidosis (DKA) 2. Outline clinical signs and symptoms of DKA leading to diagnosis 3. Describe the major metabolic changes in DKA 4. Understand the fluid and electrolyte changes in DKA 5. Discuss the major objectives of medical management of DKA 6. Provide strategies for prevention of DKA Learning Objectives: Simulation Lab Practicum 1. Recognize the clinical signs and symptoms of diabetic ketoacidosis (DKA) 2. Describe the changes in vital signs caused by diabetic ketoacidosis 3. Implement therapy in a simulated environment 4. Describe how the bio-chemical abnormalities lead to clinical signs and symptoms TIMING: First 15 minutes: Second 15 min: Third 15 min: Fourth 15 minutes: Welcome and introduction to Sim Lab and simulator History and Physical examination Initial therapy and diagnosis Definitive therapy based on underlying biochemical abnormalities First 15 minutes: Welcome and introduction Introduce the Sim Lab and the Simulator Multi-disciplinary facility Pulses, eyes blinking, pupils constrict, gas moves in and out of mouth (place hand over mouth), lungs move up and down (demonstrate chest movement) Introduce the monitor (normal values as per table below) From top to bottom of screen – mention range of normal values ECG leads II & V, arterial BP, CVP, SPO2, capnograph, respiratory rate, Introduce the lesson plan (as on bottom of first page i.e. four 15 min intervals) Heart rate beats per min Blood pressure mmHg systolic / diastolic (mean) BP CVP cmH2O central venous pressure SPO2 % pulse Ox EtCO2 mmHg End-tidal carbon dioxide concentration Respiratory rate breaths per min Normal Values DKA After Therapy 71 120/52 (80) 127 95/53 (71) 70 120/50 (80) 8 8 100 0 negative inspiration 95 100 40 30 39 12 24 14 Work (top to bottom on the monitor screen) through the normal values on the table Ask Simulator Operator for the next “State” – DKA Give the history (on the next page), as the mathematical models “settle” to their new values Second 15 min: Give the history: - History and Physical examination Tiffany has just been taken to the Emergency Department from her soccer game. She is a 25 year old female who was driven to the Emergency Department by her boyfriend, Adam. She had developed nausea, extreme fatigue, mild disorientation and blurred vision toward the end of the soccer match. Start the diabetic keto-acidosis “state” on the simulator Ask the students to point out any changes on the simulator (clinical examination) Feel pulses and count Tachycardic 120 bpm Look at chest and count Tachypneic 34 breaths/min (rapid deep respiration - Kussmaul breathing - with scent of acetone) Chest Breath sounds present bilaterally Cardiac S1 and S2 Within Normal Limits; no S3/S4 or murmurs Lungs Clear without wheezes or rhonchi Abdomen The abdominal examination revealed diffuse mild epigastric tenderness to deep palpation, but not rebound tenderness nor guarding (This is not an uncommon occurrence in DKA that appears to result from gastric stasis and distention, and resolves with treatment. The examination does not indicate acute appendicitis. Extremities No cyanosis, clubbing or edema; pulses equal Ask the students to point out any changes in the vital signs (monitor parameters) The students will have all these values in their hand-outs Feel pulse and count EKG Hypotensive CVP Pulse Ox Tachypneic ETCO2 Temperature Tachycardic 120 bpm Normal EKG complexes 90/30 mmHg low (0-2 cmH2O) CVP is NOT a learning objective – do not get side tracked 95-97% Decreased for a young, healthy, non-smoker 34 breaths/min digital number 21 – 25 mmHg 37.1 oC (98.5 oF) not on monitor Ask one of the students to talk to the patient (in an attempt to elicit the following information): Tiffany is currently lethargic and slightly confused, but can respond to questioning. She moans and asks what’s happening to her? Despite her acknowledged nausea, she still claims to be extremely thirsty. Patient also volunteers that she has diabetes (speeds up getting the history) Possible questions: we want to focus on diabetes, not on a full “coma” differential diagnosis. Any history of diabetes or insulin therapy ? Yes 40u Have you had unexplained weight loss recently? Yes 20 lbs Have you experienced increased thirst, appetite, or urination recently? Yes, multiple times per day and night Are you taking any drugs? No Make the comment about: “First look at the patient, then read the monitors” Third 15 min: Initial therapy and diagnosis Ask students what they would do next (based on vital signs) discuss in any sequence Start intra-venous infusion (IV) Give fluids for low blood pressure and tachycardia Pass around the I/V equipment I/V cannulae, infusion tubing, Ringer’s Lactate, Normal Saline Do not get side tracked with R/L and saline differences – not a learning objective Give oxygen by mask or nasal cannulae Pass around the oxygen equipment nasal cannulae for oxygen, oxygen masks open the oxygen bottle – demonstrate the “hiss” - close the oxygen tank Note to students: some emergency therapies are given even before a diagnosis is made such as oxygen therapy and IV fluids Do a urine dipstick test - on simulated urine Demonstrate the urine dipstix test Pass around the Dipstix and color code on the Dipstix bottle Do a blood glucose measurement - on simulated blood Perform a glucose test on the simulated blood Pass around the measuring equipment with the result might be electronic device, might be labStix and the color coded bottle Smell the “ketones” in the container Plan A: Sprinkle a few drops of fresh simulated ketones on the cotton wool in the container Pass around the container with the cotton wool / gauze with the liquid on it Plan B: Tear open methyl alcohol and ketone (nail polish remover) swabs Place in containers marked A and B (under the cotton wool) Pass around for the “sniffing” test Fourth 15 minutes: 5 min Definitive therapy based on underlying biochemical abnormalities - the students have actually done the background reading – this is refresher only – NOT an in-depth discussion - the discussion should focus on the relationship between the biochemistry and the clinical signs and symptoms e.g. hyperosmotic state leads to dehydration leads to hypotension and tachycardia Ask the students for a diagnosis Ask why Tiffany is dehydrated? Results primarily from osmotic diuresis due to hyperglycemia (exceeds Tmax for renal glucose reabsorption and secondarily from vomiting.) The hyperglycemia also initially causes the movement of water out of cells, with subsequent intracellular dehydration, extracellular fluid expansion and hyponatremia. Hyperglycemia also leads to a diuresis in which water losses exceed sodium chloride losses. Urinary losses then lead to progressive dehydration and volume depletion. Ask what are other signs and symptoms of dehydration? Depends upon degree of dehydration do NOT focus on numbers and percentages 3% decrease in total body water [TBW]) - dehydration just clinically detectable mild, 5% - dry mucous membranes, reduced skin turgor moderate, 7.5% - above with sunken eyes, poor capillary return severe, 10% - severely ill with poor perfusion, thready rapid pulse Ask why the acidosis develops? Due to ketonemia from overproduction of ketone bodies; also if tissue perfusion is low, from the reduction in blood flow, then some of the acidosis may be due to anaerobic production of lactate. Ask why the respiration is rapid and deep (Kussmaul)? Compensatory respiratory response to the metabolic acidosis; this may also contribute to dehydration (insensible water loss) Ask what is the rationale for inpatient treatment? The need for IV fluids, insulin and K+. (also ask why the K+ is decreased – can be asked here or earlier e.g. with dehydration) 5 min Show recovery of the patient after fluid treatment Demonstrate on simulator and monitor (Students have the value on page 2 of their hand-out) 5 min Summary and questionnaire completion: Clinical manifestations and therapy are based on the underlying biochemical abnormalities (this is the message that the developers wanted to get across – drawing a line from the sub-cellular states to the clinical manifestations) Introduction to DKA: (This is an extract from note from PBL session used by participants during the preceeding study of this case.) DKA is an acute (rapid onset), major, life-threatening complication of diabetes with a morality rate of approximately 5%. DKA is always caused by insulin deficiency, either relative or absolute (12-24 h of insulin deficiency can cause dehydration and electrolyte imbalances). DKA occurs in patients with type 1 diabetes, but is not uncommon in some patients with type 2 diabetes (90% and 10%, respectively). In an established patient, DKA usually results from failure to take insulin (most common) or acute stress (e.g., trauma, febrile illness). DKA is defined clinically as an acute state of severe uncontrolled diabetes that requires emergency treatment and intravenous (IV) fluids. Biochemically, DKA is characterized as an increase in the serum concentration of ketone bodies (beta-hydroxybutyrate and acetoacetate) and a blood glucose level of >200 mg/dL. Because the ketones must be neutralized, the buffering capacity of the blood becomes exhausted which results a reduction of blood pH (< 7.2) and serum bicarbonate (< 15 mEq/L). Additionally, there is laboratory evidence of glucosuria and ketonuria. Patient Values Upon Admission: (from original PBL session) Arterial blood gases (ABGs) Patients’ value pH pCO2 (mmHg) pO2 (mmHg) HCO3 meq/L Plasma osmolality (mOsm/kg) Serum glucose (mg/dL) Na+ (mEq/L) K+ (mEq/L) Cl- (mEq/L) BUN (mg/dL) 7.15 15 90 5 340 720 139 5.5 112 74 Normal value 7.35-7.45 35-40 75-100 22-25 280-296 74-106 136-145 3.5-5.0 96-107 8-25 Goal of treatment: (because of time limitations this will not be covered, but is provided for background) Correction of volume depletion, improved tissue perfusion, normalization of serum glucose, reduction in serum ketones, and attention to electrolyte balance are the cornerstones of therapy. Profound volume depletion is rule, not exception. A) Therefore the initial priority is restoration of ECF volume by IV infusion of normal saline (rate and composition is not important). B) Repletion of K should begin before insulin or at the same time as insulin infusion (because of total body K depletion and insulin-stimulated K uptake by muscle). C) Administer insulin. Once rehydration fluids and K are started, blood glucose will begin to fall. However, it is essential to give insulin to switch off ketogenesis and reverse the acidosis. D) HCO3 therapy is generally not recommended; the low serum bicarbonate will resolve with the decrease in ketone body production and a decrease in compensatory hyperventilation. Summary: Clinical manifestations and therapy are based on the underlying biochemical abnormalities End of hand-out for students