Diabetic Ketoacidosis in Children
advertisement

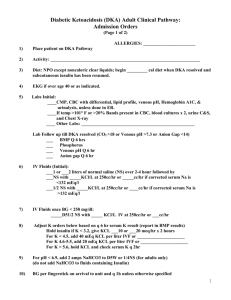
Diabetic Ketoacidosis in Children Keystone, July, 2008 Arleta Rewers MD, PhD Robert Slover MD Overview • Review the incidence and • • • pathophysiology of DKA Define the role of patient selfmonitoring including blood ketones testing and the healthcare professional advice in preventing DKA Describe current approaches to the clinical diagnosis of DKA, including the role of ketone body levels List treatment options for DKA Definition • Hyperglycemia BG > 200 mg/dl (11 mmol/l) (young or partially treated children, pregnant adolescents may present with “euglycemic ketoacidosis”) • Venous pH <7.3 and/or bicarbonate <15 mmol/L – mild DKA pH <7.3 bicarbonate <15 – moderate pH <7.2 bicarbonate <10 – severe pH <7.1 bicarbonate < 5 • Glucosuria and ketonuria/ketonemia (βHOB) Incidence of DKA at onset • Wide geographic variation in DKA rates at diabetes onset: 15 -70% • More common in developing countries • DKA rates inversely related to incidence of type 1 diabetes Diabetic Ketoacidosis at Diagnosis of DM in Youth: The SEARCH for Diabetes in Youth Study Incidence of DKA at the time of diagnosis • SEARCH is multicenter study • In 2002 began population-based ascertainment • • • • of incident cases of DM in youth younger than 20 years Incidence: Overall - 25.5% (CI 23.9-27.1) Type 1 - 29.4 % ( CI 27.5-31.3%) Type 2 - 9.7% ( CI 7.1-12.2) Rewers A et al., Pediatrics, May 2008 Risk factors for DKA at onset • Age <12 yrs • No first degree diabetic relative • Lower socioeconomic status • High dose glucocorticoids, atypical antipsychotics, diazoxide and some immunosuppresive drugs • Poor access to medical care • Uninsured Prevalence of hospitalization and DKA at onset Colorado children, 1978-2001 100% p<0.00001 80% 60% 40% % hospitalized % with DKA p=0.038 20% 0% 1978-82 n=305 1984-88 n=541 1998-01 n=606 Rewers et al., ADA 2003 DKA in children with established T1DM • The risk of DKA varies from 1:10 to 1:100 • • • • • • /p-yr Poor metabolic control or previous DKA risk Adolescent girls Children with psychiatric disorders, including those with eating disorders Lower socio-economic status Lacking appropriate insurance Inappropriate interruption of insulin pump therapy Predictors of Acute Complications in Children With Type 1 Diabetes A Rewers, HP Chase, T MacKenzie, P Walravens, M Roback M Rewers, RF Hamman, G Klingensmith 2002;287:2511-2518 Cohort of 1,243 diabetic children from BDC - age 0-19 years - residence in the six-county Denver area - outpatient visits between 1/1/1996 - 1/1/2001 Average follow-up Total follow-up DKA events DKA incidence 3.2 years 4,000 person-years 320 8 / 100 person-years Incidence of DKA in established patients BDC Cohort, 1996-2001 Incidence /100 p-yrs 15 p=0.0006 p=0.006 10 p=0.06 girls boys 5 0 <7 7 to 12 >12 Age [years] Proportion of Children with Recurrent DKA 5% • 60% of DKA episodes occurred in 5% of children who had 2 or more events 0 1 2+ # of DKA events Diabetic KetoAcidosis (DKA) 1. 160,000 Admissions to private hospitals/year 2. Cost = over 1 billion $ annually 3. 65% = <19 years old 4. Main cause of death in children with diabetes (approximately 85%) 5. Cerebral edema in 69% Cost of hospitalization of a diabetic patient $12,000 $11,123 $10,000 $8,000 $6,055 $6,000 $4,000 $2,000 $0 w ith DKA w /out DKA *HCIA-Sachs, 1998 Claims Data Warehouse, represents 2.5MM lives and 150 health plans Diabetes Care 2006 29:1150-1159 Signs of DKA • • • • • • • • • Vomiting Increased urination Abdominal pain Fruity odor to breath Dry mouth and tongue Drowsiness Deep breathing Coma Death Mortality in Children with DKA • • • • • 0.15% USA 0.18% Canada 0.31% UK 80% of deaths occurs in association with signs of CE Other causes: – hypokalemia / hyperkalemia – thrombosis – intracranial bleeding, infarction – sepsis and other infections, e.g., mucormycosis – aspiration pneumonia – pulmonary oedema, ARDS Physical Exam • Perfusion • Vital Signs - including weight • Hydration • Mental Status • Evidence for insulin resistance Initial Laboratory Evaluation Glucose* Ketones* Sodium Potassium Chloride HCO3 • Venous pH • BUN • Serum Osmolality • Phosphorus • Calcium • Anion Gap *Always perform in an ill child Calculations Serum Osmolality: 2[Na+K]+ (glucose/18) + BUN/2.8 Serum Na: Corrected Na = measured Na + (1.6)(glucose - 100)/100 Anion Gap: [Na] – ([Cl]+[HCO3]) Normally 12+/-2 mmol/L Cerebral Edema Major cause of death in childhood DKA – 20% with cerebral edema die – 20% with mild to severe neurologic outcomes • At risk: – Initial pH < 7.1 – Baseline mental status abnormal – Newly diagnosed, < 5 years old – Rapid rehydration (> 50cc/ kg in first 4 hrs) – Hypernatremia/ persistent hyponatremia Age distribution of affected children Timing of Onset of Cerebral Edema in DKA 16 14 12 # of 10 patients 8 6 4 2 0 0-2.9 3-5.9 6-8.9 9-11.9 12-14.9 12-15 >15 Time of onset of Neurological Compromise (hours) Muir A, et al, Diab Care. July 2004 Symptoms and signs of cerebral edema • Headache • Decreased or worsening level consciousness Slowing of the HR Increase in BP Sudden onset/return of vomiting of • • • • Warning signs occur before the onset of CE Clinical Factors Associated with Cerebral Edema • Prolonged Illness • Severe acidosis - low PA CO2 • Severe dehydration • Bicarbonate therapy • Persistent hyponatremia • Excessive fluid admistration Cerebral edema • CE occurs in 0.3%- 1% of all episodes of DKA • • • • Initial 24 hours of treatment Younger children (< 4 yrs) Delayed diagnosis Greater dehydration and acidosis, lower pCO2 • Insulin given before fluids Etiology of CE • Vasogenic - excessive accumulation of water and solutes in the interstitial space, due to dysfunction of the blood-brain barrier • Cytotoxic - excessive accumulation of water and solutes in the intracellular space, due to dysfunction of cell-volume regulatory mechanisms • Both forms may co-exist Excessive Free Water • Corrected Na = Na(measured)+1.6 (glucose-100)/100 • Calculated sodium is low and falling in many cases of cerebral edema • ADH levels rise 5-50 times in DKA and contribute to increase in free water and hyponatremia Cerebral Edema • Know what to look for – Altered mental status/ severe headache – Recurrence of vomiting – Changes in pupil size, seizures, bradycardia – Clinical worsening despite improving lab values – CT/ MRI changes may not be seen in early cerebral edema Cerebral Edema Bedside Score Caveat – note that patient needs to be significantly affected to meet diagnostic criteria Muir Diab Care 2004 27:1541-46 Timing of presentation of cerebral edema Treatment of cerebral edema – Mannitol: 1 gram/ kg IV over 30 minutes – Elevate the head of the bed – Decrease IVF rate and insulin infusion rate – Pediatric ICU management – Do not delay treatment until radiographic evidence Diagnosis and prevention of DKA in outpatients Why do ketones develop? No carbohydrate intake • fasting • gastroenteritis • Atkins diet, neonates fed high-fat milk Prolonged exercise, pregnancy Lack of insulin activity • onset of diabetes (insufficient secretion) • interruption of insulin delivery in established pt Increase in insulin resistance • infection, illness, surgery, stress Alcohol, salicylate ingestion, inborn metabolic errors Treatment of Mild DKA to Prevent Progression: Key: Early Detection Check blood ketones (-OHB) for a person with diabetes any time: 1) A SMBG is >300 mg/dL (16.7 mmol/L) 2) An illness or infection is present 3) Unusual symptoms are present 4) It is realized a shot/bolus was missed or bad insulin Old Paradigm: Check urine ketones New Paradigm: Check blood -OHB 1) Blood -OHB tells you how you are doing at the time of the test. (Urine may have been in bladder for hrs) 2) Urine ketone levels may not accurately reflect the severity of the ketonemia 3) A person may not be able to void 4) Some (teens) give false urine test results Hand-held device Abbott/MediSense Disadvantages to Urine Ketone Testing The results are not real time The readings are qualitative: color comparisons indicating high, medium or low levels Short shelf life (typically 90 days on opening a vial) Sulfhydryl drugs, including the ACE inhibitor, Captopril, may cause false-positive results High doses of Vitamin C may cause false-negative results Method does not detect the major ketone body hydroxybutyrate Interpretation of Blood -OHB -OHB level (mmol/L): < 0.6 = normal >1.0 = hyperketonemia 0.6-1.0 = take extra insulin + fluids 1.0-1.5 = as above; recheck in 1 hr and, if no improvement, call diabetes provider 1.5-3.0 = call diabetes provider STAT > 3.0 & sick = KETOACIDOSIS > Go to ED Sick Day Management: A Randomized Clinical Trial Laffel L, et al. Diabet Med 2005 • 123 participants, age 3–22 years – 61 randomized to home blood ß-OHB testing – 62 randomized to home urine Ketostix® testing • All participants trained on their sick-day guidelines • Outcomes – ER visits – Hospitalizations Patients who monitor blood ß-OHB test more often than those who test for ketonuria Laffel L, et al. Diabet Med 2005 Lower incidence rates of ER use/hospitalizations in patients using blood ß-OHB monitoring vs. Ketostix 6-month follow-up p = 0.05 Laffel L, et al. Diabet Med 2005 Use of Blood -hydroxybutyrate Levels at the Bedside During Treatment of DKA ADA, June, 2007 Fat Normal state postprandial glucose acetyl CoA pyruvate Krebs cycle oxaloacetate citrate Fat Normal state postprandial lipase fatty acids (+ glycerol) fatty acyl CoA glucose -oxidation acetyl CoA pyruvate Krebs cycle oxaloacetate citrate insulin Normal state postprandial Fat lipase fatty acids (+ glycerol) fatty acyl CoA -oxidation acetyl CoA Krebs cycle acetoacetyl CoA HMGCoA synthase acetoacetate 1:1 acetone -OHB insulin Ketosis in DKA Fat - alternative source of energy lipase fatty acids glucose fatty acyl CoA -oxidation acetyl CoA pyruvate Krebs cycle oxaloacetate acetoacetyl CoA HMGCoA synthase acetoacetate 1:10 citrate acetone -OHB glucagon insulin Is bedside β-OHB monitoring using hand-held device as accurate as reference laboratory method ? Correlation between venous whole blood β-OHB levels measured using Precision Xtra™ and serum levels using Cobas Mira Plus (Roche) Laboratory reference β-OHB [mg/dL] Bedside meter β-OHB [mmol/L] Rewers A et al. Diabet Technol Therapeutics, 2006;8:671 Bland-Altman plot showing good agreement between β-OHB levels measured using Precision Xtra™ and Cobas Mira Plus (Roche) Mean difference = 0.18 (C.I. -1.18-1.53) Rewers A et al. Diabet Technol Therapeutics, 2006;8:671 also Byrne H, et al. 2000; Wallace TM, et al. 2001 Ham MR, et al. 2004; Khan ASA, et al. 2004 CONCLUSION Real-time bedside measurement of OHB is generally as accurate as reference laboratory, especially at levels up to 3.0- 4.0 mmol/L Is capillary blood β-OHB monitoring superior to testing urine for ketones ? Measurement of Ketones • Urine ketone measurements use a “dip stick” method based on a chemical reaction with acetoacetate. E.g., Chemstrip® from Roche; Clinistix®, Ketostix® , Keto-Diastix® from Bayer) • Blood ketone testing that specifically measures ßhydroxybutyrate are available for use in the laboratory (e.g., Sigma®, Cobos® from Roche) and a hand-held meter (Abbott / MediSense) Blood β-OHB testing is superior to urine ketone testing in detecting ketosis Sensitivity Specificity Positive predictive value Ketonuria 63% 100% 100% 72% Capillary blood β-OHB 80% 100% 100% 83% Gold standard – plasma β-OHB by reference laboratory method (KONE Delta Automatic Analyzer) Guerci B , et al. Diabetes Care 2003 Similar data: Taboulet P et al. Eur J Emerg Med 2004 Negative predictive value Advantages Blood β-OHB vs. Urine Ketone Testing • -OHB is a better marker of ketosis than acetoacetate • -OHB is ‘real-time’ while ketonuria is usually ‘old news’ • Ketonuria doesn’t accurately reflect severity of ketonemia • A dehydrated person may not be able to void • Some people are too ill or exhausted to do the urine test • Some patients (teens) give false urine sample • Urine ketone strips spoil after opened >6 months -hydroxybutyrate is a better indicator of metabolic status when detecting and treating DKA Schade DS, Eaton RP Special Topics in Endo and Metab 1982;4:1-27 β-OHB in diagnosis of DKA in ED β-OHB helps to diagnose DKA in patients with known or new diabetes seen in ER N Blood β-OHB BG>200, adults 139 >0.42 Diabetic children 55 >1.5 BG>250, age>18 160 >1.8 91% BG>200, age >15 50 >2.0 >3.0 100% 100% Patients Study Bektas, 2004 Ham, 2004 [mmol/L ] Sensitivity Specificity PPV 72% NPV 82% 85% 100 % 92% 86% 95% 85% 88% 60% 64% 100 % 100 % Nauheim, 2006 Harris,2004 Capillary blood β-OHB vs. venous pH in 118 newly diagnosed children no DKA DKA compensated acidosis 3 0.5 7.25 Prisco F, et al. Pediatr Diabetes 2006 Can bedside β-OHB monitoring replace repeat measurements of pH, bicarbonate and pCO2 during treatment of DKA? Correlation between baseline β-OHB and other biochemical indicators in 68 children with DKA Pearson correlation coefficients (p <0.05 for all) Biochemical indicator pH Bedside meter -0.63 Reference method -0.74 Bicarbonate -0.74 -0.80 pCO2 -0.55 -0.61 Glucose 0.57 0.63 BUN 0.35 0.42 Rewers A et al. Diabet Technol Therapeutics, 2006;8:671 Time series analysis showing that bedside β-OHB levels correlated very closely with time-dependent levels of venous blood gases Biochemical indicator pH Bedside meter β -6.3 ** Reference method β -8.0 ** Bicarbonate β -0.22 ** β -0.24 ** pCO2 β -0.04 * β -0.05 ** * p<0.001; ** p<0.0001 Rewers A et al. Diabet Technol Therapeutics, 2006;8:671 CONCLUSION While the initial measurement of pH, bicarbonate and pCO2 is warranted, realtime bedside measurement of -OHB may replace repeat measurements of blood gases in treatment of DKA Can bedside β-OHB monitoring shorten duration of DKA treatment ? In most newly-diagnosed children with ketosis, capillary ketonemia resolves sooner than ketonuria N =99 Prisco F, et al. Pediatr Diabetes 2006; In children with DKA, capillary ketonemia resolves on average 11 hours sooner than ketonuria (n=40) Example of an individual treatment profile pH >7.3 β-OHB <1.0 pH >7.3 No ketonuria i.v. insulin U kg/h β-OHB Noyes KJ, et al. Pediatr Diabetes 2007, confirming Vanelli M, et. Al. Diabetes Care 2003 CONCLUSIONS Real-time bedside measurement of OHB may help to optimize treatment of DKA and shorten the duration of hospitalization Initial Laboratory Evaluation Glucose* Ketones* Sodium Potassium Chloride HCO3 • • • • • Venous pH BUN Serum Osmolality Phosphorus Calcium *Always perform in an ill child Treatment Monitoring • Management requires close attention to detail • Use a flowsheet to track vital signs labs, rates of insulin, fluids, dextrose • Neurological status – consider neuro checks q 1 hr – How does the patient look TO YOU? • Assess, reassess and then assess again Treatment • Consider ICU admission for closer monitoring if: • – Severe DKA (pH < 7.1 or < 7.2 in young child) – Altered level of consciousness – Under age of 5 years – Increased risk for cerebral edema Caution with meds that may alter mental status Fluid Therapy for DKA • Assume 10-15% dehydration • Begin with a 10-20 ml/kg bolus of NS • Replace calculated deficit evenly over • 36 hours - generally 1.5 x maintenance for the next several hours is appropriate Do not exceed 40ml’s/kg in the initial 4 hours, or 4 L/m squared in 24 hours DKA - Fluids • Double bag system – ¾ NS at 1.5 x M until glucose below 300 mg/dl – D10 ¾ NS to be mixed with ¾ NS to achieve desired glucose concentration – K supplementation 20mEq/L K Acetate + 20mEq/L K Phosphate – Ionized calcium is low, phosphorous should not be given – early replacement and frequent monitoring – Bicarbonate therapy is rarely, if ever, indicated Insulin Therapy for DKA • IV infusion with basal rate 0.1 U/kg/hr • No initial insulin bolus – it will decrease time to correction of the glucose, but does not alter the time to correction of acidosis It may decrease the serum osmolality more rapidly than desirable • Ideal glucose decline is about 100 mg%/hr • Continue insulin until urinary (blood) ketones are cleared Potassium • Add potassium when K< 5 and with urination – K >5.5 – no potassium in IVF – K 4.5 – 5.5 – 20 meq/L K+ – K <4.5 – 40 meq/L K+ Phosphate – the controversy • Prevent depletion of RBC 2,3 DPG which will improve tissue oxygenation as acidosis is resolving • May be useful in patients with anemia, CHF, pneumonia, hypoxia Use of Bicarbonate in DKA • Bicarbonate should be used only when there is severe depression of the circulatory system or cellular metabolism... • Not recommended unless pH <7.0, not even then, unless above true DKA: Cases • 12 year old admitted with: – pH = 7.0 – Na= 136, K=3.8, glucose 583mg/ dl – She is oriented and conversant on admission, you follow the DKA protocol, • 2 hours later she becomes difficult to arouse and • is responsive only to deep pain. - What do you do? Presume cerebral edema – Decrease fluid infusion to insensible losses – Give mannitol: 1 gm/kg DKA: Cases • 6 y/o boy is admitted in severe DKA. The • • • family has been traveling and he has been ill for several days. Initial pH=7.0, K+ = 3.7, glucose is 350mg%. Despite replacement, his K+ now is 1.9 mg/dl - what do you do? A “bolus” of potassium at TCH is actually an infusion over an hour. An actual bolus of potassium into a central vein may be lethal DKA: Cases • 16 year old boy is admitted in moderate to • severe DKA (pH=7.23), his weight is 230 lbs, his BG is 1400, serum osm is 360 mOsm/L, what do you do? Monitor! Everything you can! Successful Management • Careful attention to detail • Careful record keeping – A detailed flow chart is essential – Following the data recorded is also essential • Repeated examination of the patient