gp referral proforma for suspected
advertisement

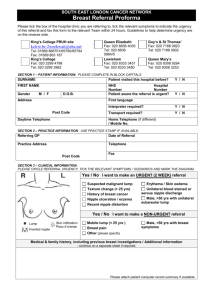
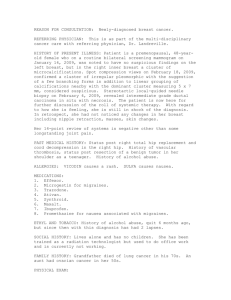
GP REFERRAL PROFORMA FOR ALL BREAST SYMPTOMS PLEASE USE 2WW SERVICE ON CHOOSE AND BOOK OR FAX TO 01823 343 417 (MPH) OR 01935 384 640 (YDH) Decision to refer date (to be completed by GP): Do you suspect that this patient may have cancer? Referral received date (to be completed by hospital): Yes No (Must be completed) Please note: All breast referrals are now mandated to be seen within 14 days of receipt of referral and thus patients should be made aware they will receive an appointment within this timescale. Ticking the above box indicates an increased suspicion of cancer and should be completed for those patients who you consider may have a breast cancer, this is important as these patients will be tracked against the National Cancer Waiting Times Target. If yes: Has the patient been informed that they are being referred for suspected cancer? Has the patient been given the 2WW referral patient information leaflet? Dates patient is unavailable in next 14 days: Patient Details: Referring GP Details: Surname: NHS No: Name: Forename: Hosp No: Address: Practice: Post Code: DOB: Yes Yes No No Telephone No: Fax No: E-mail Address: Daytime Tel No: Mobile Tel No: Mammogram in last 3 years? Yes / No Location? Date? Re-Referral? Yes / No Date Last Referred Family history of breast cancer? If Yes, please specify: Yes No SYMPTOMS (please tick all that apply): Any age with a lump Any age with breast pain Any age, with previous breast cancer, who present with a further lump or suspicious symptoms Unilateral eczematous skin or nipple Nipple distortion Spontaneous nipple discharge Males with a firm subareolar area mass Abscess Recurrent cyst If you wish to refer for any of the following: family history surveillance, reconstruction, or High Risk Breast Cancer Surveillance (e.g. previous high risk lesions such as LCIS, ADH, previous mantle radiotherapy or family history / mutation carriers) Please tick here only and refer direct to the following locations: Breast Care Centre for MPH referrals or Fax to 01935 384 640 for YDH referrals Please attach* additional clinical details to include: significant medical history and co-morbidities current medication clearly indicating if the patient is receiving any anti coagulation therapy. recent blood results and any other relevant information * Please note that referrals received without adequate supporting clinical information cannot be processed and will be returned to the referrer as incomplete Document1