primary health care
advertisement

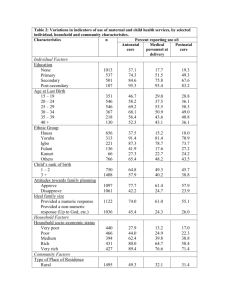
“Health For All’’ Dr.Ramesh Pawar Moderated By: Dr.Ranjan Solanki. Framework Introduction Atma-ata declaration Primary Health care National Health Policies 1983 and 2002 Progress and Achievements Challenges Success Stories. References. What is Health? A state of complete physical, mental, and social well being and not merely absence of disease or infirmity. What does health for all means? “Large numbers of the world’s people, perhaps more than half, have no access to health care at all, and for many of the rest the care they receive does not answer the problems they have.” John Bryant in his book “Health and the Developing World The Joint WHO – UNICEF international conference in 1978 at Alma-Ata (USSR) Declared that “the existing gross inequalities in the status of health of people particularly between developed and developing countries as well as within the countries is politically, socially and economically unacceptable.” ample evidence of a dysfunctional, nonperforming public health system. …The situation varies across the country and in some parts of the country it functions very well. I think on an average, it does not function well and there are some parts where it is really functioning incredibly badly Montek Singh Ahluwalia Dy Chairman, Planning Commission HEALTH FOR ALL ATTAINMENT OF A LEVEL OF HEALTH THAT WILL ENABLE EVERY INDIVIDUAL LEAD A SOCIALLY AND ECONOMICALLY PRODUCTIVE LIFE The 30th World Health Assembly in May 1977 resolved “The main social target of governments and WHO in the coming decades should be the attainment by all citizens of the world by the year 2000 AD of a level of health that will permit them to lead a socially and economically productive life.’’ HEALTH FOR ALL BY 2000 AD The Joint WHO – UNICEF international conference in 1978 at Alma-Ata (USSR) Alma-Ata Declaration called on all the governments to formulate national health policies according to their own circumstances to launch and sustain primary health care as a part of national health system. The Alma-Ata conference called for acceptance of the WHO goal of HEALTH FOR ALL by 2000 AD and ‘Primary Health Care’ as a way to achieve Health For All Alma –ata declaration Health is a fundamental human right and that the attainment of the highest possible level of health is a most important worldwide social goal. The existing gross inequality in the health status of the people particularly between developed and developing countries is politically, socially and economically unacceptable. Economic and social development, based on a new international economic order is of basic importance to the fullest attainment of health for all. The people have the right and duty to participate individually and collectively in the planning and implementation of their health care. Alma –ata declaration Government have a responsibility for the health of their people which can be fulfilled only by the provision of adequate health and social measures. All government should formulate national policies, strategies and plans of action to launch and sustain primary health care. All countries should cooperate in a spirit of partnership and service to ensure PHC for all people. An acceptable level of health for all the people of the world by the year 2000 can be attained through a further and better use of the world’s resources. The Alma-Ata conference defined that “Primary health care is an essential health care based on practical, scientifically sound and socially acceptable methods and technology, made universally accessible to individual and families in the community, through their full participation and at a cost that the community and the country can afford”. Principles of primary health care 1.Equitable distribution 2.Community participation. 3.Inter-sectoral coordination 4.Appropriate technology 1. Equitable distribution Some thing for all and most for those who need the most “Bahujan hitae bahujan sukhae” 2. Community participation There must be a continuing effort to secure meaningful involvement of the community in the planning, implementation and maintenance of health services, besides maximum reliance on local resources such as manpower, money and materials 3.Intersectoral coordination "primary health care involves in addition to the health sector, all related sectors and aspects of national and community development, in particular agriculture, animal husbandry, food, industry, education, housing, public works, communication and others sectors". 4. Appropriate technology "technology that is scientifically sound, adaptable to local needs, and acceptable to those who apply it and those for whom it is used, and that can be maintained by the people themselves in keeping with the principle of self reliance with the resources the community and country can afford" Elements of primary health care 1.Education concerning prevailing health problems and the methods of preventing and controlling them 2.Promotion of food supply and adequate nutrition 3.An adequate supply of safe water and basic sanitation 4.Maternal and child health care including family planning 5.Immunizat ion against the major infectious diseases 6.Preventio n and control of locally endemic diseases 7.Appropriat e treatment of common diseases and injuries 8.Provision of essential drugs National strategy for health for all ...... As a signatory to alma- ata declaration in 1978, the Govt. Of India was committed to taking steps to provide HFA to its citizens. In this connection two important reports appeared: Report of study group on “HEALTH FOR ALL – on alternative strategy” sponsored by Indian council of social science research (ICSSR) and Indian council of medical research( ICMR) Reports of working group on “HEALTH FOR ALL by 2000 A.D. ’’ sponsored by Ministry of health and family welfare, Govt. Of India. This health policy forms a basis of the national health policy formulated by ministry of health and family welfare, Govt . Of India in 1983. National Health Policy -1983 NHP 1983 stressed the need for providing primary health care with special emphasis on prevention, promotion and rehabilitation Suggested Planned time bound attention to the following 1.Nutrition, prevention of food adulteration. 2.Mainatince of quality of drug 3.Water supply and sanitation 4.Environmental protection 5.Immunisation programme 6.Maternal and Child Health Services 7.School Health Programme 8.Occupational Health National Health Policy 1983…… India had its first national health policy in 1983 i.e. 36 years after independence. For better programme planning NHP 1983 recommended an effective Health Information System. NHP 1983- Goal suggested/achieved NHP 1983- Goal suggested/achieved Differentials in health status among rural/urban India Differentials in health status among states Differentials in health status among socio-economic groups Achievements Through The Years 1951-2000 Achievements Through The Years 1951-2000 Achievements Through The Years - 1951-2000 But by the end of 2000 century it was clear that the goals of health for all by the year 2000 AD would not be achieved ...... Factors responsible for this failure were: Biased and poor socio- economic development in the region where it was needed most. Discriminatory policies due to age, gender and ethnicity thus preventing access to health care surveillance. Millennium Development Goals Millennium Summit held in September 2000 in New York Representatives from 189 countries met to adopt the United Nations Millennium Declaration Poverty eradication and development by 2015 being the core issue “Millennium Development Goals” Millennium Development Goals 8 goals 18 targets 48 indicators Related to health •3 goals •8 targets •18 indicators National Health Policy 2002 Objectives: Achieving an acceptable standard of good health of Indian Population, Decentralizing public health system by upgrading infrastructure in existing institutions, Ensuring a more equitable access to health service across the social and geographical expanse of India. NHP 2002, Objectives…….. Enhancing the contribution of private sector in providing health service for people who can afford to pay. Giving primacy for prevention and first line curative initiative. Emphasizing rational use of drugs. Increasing access to tried systems of Traditional Medicine Goals – NHP 2002 1. Eradication of Polio & Yaws-2005 2. Elimination of Leprosy-2005 3. Elimination of Kala-azar- 2010 4. Elimination of lymphatic Filariasis- 2015 5. Achieve Zero level growth of HIV/AIDS-2007 Goals – NHP 2002.... 6.Reduction of mortality by 50% on account of Tuberculosis, Malaria, Other vector and water borne Diseases-2010 7.Reduce prevalence of blindness to 0.5%-2010 8. Reduction of IMR to 30/1000 & MMR to 100/lakh -2010 9. Increase utilisation of public 2010 health facilities from current level of <20% to > 75% Goals – NHP 2002.... 10.Establishment of an integrated system of surveillance, National Health Accounts and Health Statistics-2007 11.Increase health expenditure by government as a % of GDP from the existing 0.9% to 2.0%2010 12. Increase share of Central grants to constitute at least 25% of total health spending- 2010 Goals – NHP 2002.... 13. Increase State Sector Health spending from 5.5% to 7% of the budget -2005 14. Further increase of State sector Health spending from 7% to 8%-2010 NHP-2002 Policy prescriptions Financial resource 1.Increase in health sector expenditure to 6% of GDP, with 2% by public health investment by 2010 is recommended by the policy. 2.Existing 15% of central government contribution is to be raised to 25% by 2010. Suggested norms for health personnel Equity NHP 2002 has observed that the attainment of health indices has been very uneven across rural-urban divide, Differentials in health status among rural/urban India Equity….. To overcome the social inequality, NHP 2002 has set an increased allocation of 55% total public health investment for the primary health sector, 35% for secondary sector and 10% for tertiary Summation…… Crafting of a National Health Policy is a rare occasion. Allow our dreams to mingle with ground realities that needs are enormous and the resources are limited Health needs are also dynamic and keep changing over time Had to make hard choices between various priorities NHP 2002 has given a continuum to NHP 1983, where primary health care is adopted as the main strategy through Decentralization Equity Private sector/indigenous system participation Rise in public investment Summation…… The ultimate goal is achieving an acceptable standard of good health of people of India. The commitment of the service providers and an improved standard of governance is a prerequisite for the success of any health policy. Steps Towards Health For All-India 1985 – The universal immunization program (UIP) was launched to provide universal coverage of infants and pregnant women with immunization against identified vaccine preventable diseases. 1992-93 – the UIP has been strengthened and expanded into the child survival and safe motherhood (CSSM) project. It involves sustaining the high immunization coverage level under UIP, and augmenting activities under oral rehydration therapy, prophylaxis for control of blindness in children and control of ARI. Steps Towards Health For All-India 1997 – Reproductive and child health (RCH-phase1) program was launched which incorporated child health, maternal health, family planning, treatment and control of reproductive tract infection and adolescent health. 2005-2010 – RCH-phase 2 aims at sector wide, outcome oriented, program based approach with emphasis on decentralization, monitoring and supervision which brings about a comprehensive integration of family planning into safe motherhood and child health. Steps Towards Health For All-India 2005-2012 – National Rural Health Mission a major undertaking by the present united progressive alliance government. It is also from a strategic framework to implement the national health policy 2002. The NRHM subsumes key national programmes, Reproductive and child health -2 National disease control programme and integrated disease surveillance project. Trends… Trends in Maternal Deaths Levels of MMR by region,1999-2009 Under Five Mortality Rate India,1990-2009 Child deaths are falling, but not quickly to reach the MDG Goal. Infant mortality Rate(IMR)- India, 1990-2009 MGD Target…. Trends in Total Fertility Rate Replacement level TFR, Viz 2.1, has been attained by Andhra Pradesh 1.9 Delhi 1.9 Himachal Pradesh 1.9 Karnataka 2.0 Kerala 1.7 Maharashtra 1.9 Punjab 1.9 Tamil nadu 1.7 West Bengal 1.9 Distribution of Deaths in Word- 2004 Source: Global burden of disease :2004 update Projected Global Deaths: 2004-2030 Source: Global burden of disease :2004 update India Literacy Rate(1901-2011) Public health spending in select countries Achievement so far… Samll Pox Eradication: Smallpox is an acute exanthematous disease caused by infection with the poxvirus variola History of Smallpox Eradication History of Smallpox Vaccination…. 1805 Growth of Virus on Flank of a Calf in Italy 1864 Publicity about vaccine production at a medical congress. After WWI Most of Europe smallpox free After WWII Transmission interrupted in Europe and North America 1940’s Stable freeze dried vaccine perfected by collier. Small pox eradication… History of Smallpox Eradication 1950 Pan American Sanitary Organization decides to undertake eradication hemisphere-wide. 1959 World Health Assembly adopts goals to eradicate smallpox 1966 Word Health Assembly decided to intensify eradication and provide more funds History of Smallpox eradication Small pox eradication Smallpox eradication strategy Mass vaccination campaign in each country, using vaccine of ensured potency that would reach> 80% of population. Development of a system to detect and contain cases and outbreaks. Smallpox eradication Bye-bye Smallpox….. Small eradication-triumphs The Faces of Smallpox…. Guinea worm eradication… Eradication of Guinea Worm The Source: Eradication of Guinea Worm… Affected are people in rural deprived and isolated communities. Prevention Strategy Number of dracunculiasis is cases-Globally,1998-2007 Guinea worm endemic countries in 1991 and 2007 Eradication of Guinea-Worm (NGEP) The programme has been evaluated seven times by independent experts “This is a remarkable achievement made possible by active inter sectoral collaboration between the key departments of health, water supply, and rural development,” Henk van Norden, the coordinator of Water Supply—a division of Unicef—which played a crucial part in the eradication of guinea worm disease. Guinea Worm eradicated…. Polio… Successful Health Research Successful health research projects in . Region include dengue vaccine the production in Thailand, hepatitis B vaccine and anti-snake toxoid production in Myanmar, leprosy drug trials and community-based rehabilitation in India, testing drug resistance in malaria parasites in Thailand, and a multicentric study on low birth weight and its risk factors in India, Nepal and Sri Lanka Evaluation of HFA : 1979-2006 Reasons for slow progress: Insufficient political commitment Failure to achieve equity in access to all PHC components Slow socio- economic development Difficulty in achieving inter sectoral action for Health Unbalanced distribution of resources Reasons for slow progress (contd.) Weak health information systems and lack of baseline data Pollution, poor food safety, and lack of water supply and sanitation Rapid demographic and epidemiological changes Focusing on clinical services while neglecting services that reduce exposure to disease is like mopping up the floor continuously while leaving the tap running (paraphrased from Laurie Garrett, Betrayal of Trust) The Basic Requirements for Sound PHC (the 8 A’s and the 3 C’s) Appropriateness Availability Adequacy Accessibility Acceptability Affordability Assessability Accountability Completeness Comprehensiveness Continuity Obstacles to the implementation of the PHC strategy Misinterpretation of the PHC concept Lack of political will Centralized planning and management What has been considered primary care in well resourced has been dangerously over simplified in resource constrained setting PHC can provide place wide range of problems-would would not accept that low income countries could focus few “priority disease’’ PHC hub from which patients are guided through health system-it is not acceptable for low income countries to reduce to stand alone health post or isolated community health worker. Patient participation- LIC services restricted to one way delivery channel. PHC deals with Ds preventive, curative and promotive- only curative For LIC Requires adequate resources and investment then provide much better value for money-it not acceptable In LIC PHC finance out of pocket on assumption that it is cheap and should be used by poor only.. Five common shortcomings of health-care delivery Five common shortcomings of health-care delivery Inverse care: People with the most means – whose needs for health care are often less – consume the most care. Impoverishing care: Wherever people lack social protection and payment for care is largely out-of-pocket at the point of service, they can be confronted with catastrophic expenses. Over 100 million people annually fall into poverty because they have to pay for health care. Five common shortcomings of healthcare delivery… an average Indian spends a substantial amount (58%) of his total annual income for his hospital treatment. 40% of hospitalized Indians borrow or sell assets to cover hospital expenses. 25% of hospitalized Indians fall below poverty line because of hospital expenses. Impact of abolishing user fees. Source :Words health report 2008;primary health care Five common shortcomings of health-care delivery… 3.Fragmented and fragmenting care: The excessive specialization of health-care providers and the narrow focus of many disease control programmes discourage a holistic approach to the individuals and the families they deal with and do not appreciate the need for continuity in care. Health services for poor and marginalized groups are often highly fragmented and severely under-resourced, while development aid often adds to the fragmentation Aspects of care that distinguish conventional health care from peoplecentred primary care How Health system Diverted From PHC core values. Five common shortcomings of health-care delivery… 4.Unsafe care: Poor system design that is unable to ensure safety and hygiene standards leads to high rates of hospitalacquired infections, along with medication errors and other avoidable adverse effects that are an underestimated cause of death and ill-health • Lack of Health care staff. India Health Infrastructure. Five common shortcomings of health-care delivery… 5.Misdirected care: Resource allocation clusters around curative services at great cost, neglecting the potential of primary prevention and health promotion to prevent up to 70% of the disease burden. The current criticism against health care services is that they are (a) Predominantly urban oriented (b) Mostly curative in nature (c) Accessible mainly to small part of the population Commercialization of Health Care Private health care is clearly associated with profit, exploitation and preferential service to high income groups. It result in inefficient, inequitable and poor quality care. “Doctor, do you think I need an MRI?” Success stories… Success Story-1. Economic development and investment choices in health care: the improvement of key health indicators in Portugal. Portugal recognized the right to health in its 1976 constitution, following democratic revolution. Political pressure –inequalities Creation of National Health System-funded by taxation & complimented by PP insurance schemes and out –of pocket payments. System fully establish 1979-83, working on PHC principle. Eligibility-register to family physician in health center.(network great success) Life expectancy 9.2 more than 30yrs back Double GDP per capita Decreased IMR by half every eight years. Multivariate analysis on time series on various mortality indices since 1960 shows b/o PHC principles. Factors explaining mortality reduction in Portugal, 1960-2008 Success stories 2- closing the urban- rural gap through progressive expansion of PHC coverage in rural areas in the Islamic Republic of Iran. In 1970s, Iranian Govt. policies emphasized prevention as a long term investment, allocation of resources to rural and under privileged areas and prioritizing ambulatory care over hospitalization. Network of District Team formed to oversee 2500 village based rural health centers was establish. Each center staff by team-GP, midwife , nurse,several health technicians . Each rural health center has 1-5 small point of care “Health Houses’’ (17000,>90% rural population has access to heath care ) Health Houses are staffed by “Behvarz” (MPW) PHC Network grows and cover 24 million people of villages small citiesbring the pont of care closer to where people live and work Progressive roll- out of this system has hepled to reduce the urban and rural gaps in child mortality. Under-five mortality in rural and Urban areas, the Islamic Republic of Iran, 1980-2000 Success story-3 Sultanate Oman In the late 1970s, the Sultanate of Oman had only a handful of health professionals. People had to travel up to four days just to reach a hospital, where hundreds of patients would already be waiting in line to see one of the few (expatriate) doctors. All this changed in less than a generation. Oman invested consistently in a national health service and sustained that investment over time. There is now a dense network of 180 local, district and regional health facilities staffed by over 5000 health workers providing almost universal access to health care for Oman’s 2.2 million citizens, with coverage now being extended to foreign residents. Over 98% of births in Oman are now attended by trained personnel and over 98% of infants are fully immunized. Life expectancy at birth, which was less than 60 years towards the end of the 1970s, now surpasses 74 years Selected best performing countries in reducing U-5 mortality by at least 80%, by region,1975-2006 Variable progress in reducing U5 mortality, 1975-2006, in selected countries with similar rates in 1975. When supplier- induced and consumer driven demand determine medical device: ambulatory care in India. Mr.S is typical patient lives in urban Delhi. Over 70 pvt. Sector medical care providers within 15 mins walk from her house. She chooses the private clinic run by Dr.SM &his wife. Above the clinic a prominent sign says “Ms.MM Gold Medalist , MBBS’’ suggesting that the clinic is staffed by a highly proficient doctors As it turns out, Ms. MM is rarely at the clinic. We were told that she sometimes comes at 4 a.m. to avoid the long lines that form if people know she is there. We later discover that she has “franchised” her name to a number of different clinics. Therefore, Ms. S sees Dr. SM and his wife, both of whom were trained in traditional Ayurvedic medicine through a six-month long-distance course. Continue… The doctor and his wife sit at a small table surrounded, on one side, by a large number of bottles full of pills, and on the other, a bench with patients on them, which extends into the street. Ms. S sits at the end of this bench. Dr. SM and his wife are the most popular medical care providers in the neighbourhood, with more than 200 patients every day. The doctor spends an average of 3.5 minutes with each patient, asks 3.2 questions, and performs an average of 2.5 examinations. Following the diagnosis, the doctor takes two or three different pills, crushes them using a mortar and pestle, and makes small paper packets from the resulting powder which he gives to Ms. S and asks her to take for two or three days. These medicines usually include one antibiotic and one analgesic and anti-inflammatory drug. Dr. SM tells us that he constantly faces unrealistic patient expectations, both because of the high volume of patients and their demands for treatments that even Dr. SM knows are inappropriate. Continue… Dr. SM and his wife seem highly motivated to provide care to their patients and even with a very crowded consultation room they spend more time with their patients than a public sector doctor would. However, they are not bound by their knowledge […] and instead deliver health care like the crushed pills in a paper packet, which will result in more patients willing to pay more for their services FOUR SETS OF PHC REFORMS Needed for an effective response to the health challenges of today’s world UNIVERSAL COVERAGE REFORMS: systems contribute to health equity, social justice. SERVICE DELIVERY REFORMS: health services as primary care, i.e. around people’s needs and expectations. PUBLIC POLICY REFORMS: reforms that secure healthier communities, by integrating public health actions with primary care and by pursuing healthy public policies across sectors LEADERSHIP REFORMS:Reforms that replace disproportionate reliance on command and control on one hand, and laid faire disengagement of the state on the other, by the inclusive, participatory, negotiation-based leadership required by the complexity of contemporary health systems India Shinning “India is shining ok for the glossy magazines, but if you just go outside metro you will see that everything about India shining is refuted … [In the villages] alcoholism is rife and femaie infacticide and crime are rising. You have to bribe to get electricity, water. Yes, the middle and upper classes are taking off, but the 700 million who are left behind, all they see is gloom and darkness and despair. They are born to fulfil their destiny and have to live this way and die this way. The only thing that shines for them is the sun, and it is hot and unbearable and too many of them die of heatstroke.” Let us work together for “Health for ALL.’’ References Primary health care, report of the international conference on primary health care Alma Ata, USSR, 6-12 September 1978, WHO,1978. Primary health care Volume 1,2,3, PR Dutt. The Gandhigram Institute of Rural Health & Family Welfare Trust, Tamilnadu 1993. Kishor J. National health programs of India;10th ed. Detels R, MacEwan J, Beaglehole R, Tanaka H. Oxford textbook of public health, 4th edition. Oxford: Oxford university press; 2002. Agarwal S. Public Health and Community Medicine Related Policies in India. Textbook of Public Health and Community Medicine, Dept of Community Medicine, AFMC, Pune in collaboration with WHO, India office, New Delhi; 1st edition,2009. From Alma Ata to the year 2000, WHO, 1988. National Family Health Survey (NFHS) – I (1992-93), II (1998-99) Census of India 2011, Houses, Household Amenities and Assets Series: India http://www.indexmundi.com/g/r.aspx?c=in&v=2223 www.parliamentofindia.nic.in UNCTAD, E Commerce and Development Report, 2002 11, Ministry of HRD, Gol, Annual Report, 2001-02 Government of India, Ministry of HRD, Annual Report, 2001-02 Human Development Report, 2004