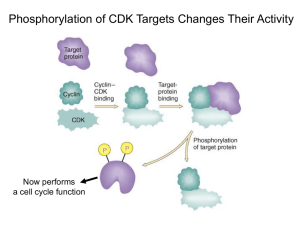
Antireplication Agents:
CDK Inhibitors and Telomerase
Inhibitors
Richard S. Finn, MD
Assistant Professor of Medicine
Geffen School of Medicine at UCLA
Faculty Disclosure
Richard Finn, MD, has disclosed that he has received fees for
non-CME services from Genentech.
Cyclin D Kinases and Cancer
CDKs are a subgroup of seine/ threonine kinases
In general very small proteins (34-40 kDa)
Bind to activating proteins: cyclins
Without cyclins, CDKs have little kinase activity
Play a key role in regulating cell cycle progression through all phases of the cell
cycle
Various cyclin/ CDK complexes act at different parts of the cell cycle
Temporal and quantitative regulation
Negative regulation by cyclin dependent kinase inhibitors (CKI)
INK 4 family (p15, p16, 18, p19
Cip/ Kip family (p21, p27, p57)
Alterations in CDKs are uncommon, compared with cyclin dysregulation
Altered regulation/ expression in many malignaices
Cyclin D1 amplification has been described in various malignancies, including
breast cancer, with variable prognostic significance
t(11;14) mantle cell lymphoma
Rb loss, a well known oncogenic event
1. Finn RS, et al. Breast Cancer Res. 2009;11:R77. 2. Lundberg AS, et al Eur J Cancer. 1999;35:1886-1894.3. Buckley
MF, et al. Oncogene. 1993;8:2127-2133. 4. Dickson C, et al. Cancer Lett. 1995;90:43-50.
Cyclin D Kinases and Cancer
Vermullen Cell Proliferation
Rb as Master-Regulator of the R Point
p16(INK4a)
Modified from Figure 8.19 . The Biology of Cancer. © Garland Science 2007.
CDK/ Cyclin Inhibitors
Targeting CDK
>50 inhibitors described
Generally in several classes
– Purine analogoues (ie roscovitine)
Selicicilib (CYC202)
CDK2/E CDk 2/A CDK7 CDK 9
– Pyrimidine analgoues
Dinaciclib (SCH727965)
CDK 2, CDk5, CDK 1, CDK 9
– Flavonoids (flavopiridol)
– Indolinones
– Staurosporine
Targeting Cyclin
cyclin expression modulators (ON013105)
CDK/ Cyclin Inhibitors
Selicicilib (CYC202)
– Phase II
Nasopharyngeal
APPRAISE Study
Randomized Phase II, NSCLCA 3rd line or greater vs BSC
Dinaciclib (SCH727965)
Phase II
– Melanoma
– AML
ON013105
Phase I- mantle cell lymphoma
PD 0332991: Background
O
The compound
N
Potent, selective, reversible inhibitor of
HN
CDK4,6
Small molecule
Oral agent
N
O
N
O
N
OH
S
O
+
The opportunity
N
O
N
H2
Potential first in class
Potential impact on hematopoietic and solid
tumors
Potential use in pediatric indications
Single-agent and combination approaches
under investigation
Finn RS, et al. Breast Cancer Res. 2009;11:R77.
PD 332991
Rb as Master-Regulator of the R Point
Target of PD 0332991
p16(INK4a)
Inactivates Rb and
allows progression
Modified from Figure 8.19 . The Biology of Cancer. © Garland Science 2007.
Sorlie et al PNAS 2001
Human Breast Cancer Cell Line Panel Can Recapitulate the
Molecular Heterogeneity of Clinical Disease
51 Human
Breast Cell Lines
25
Luminal
10
9
6
ER positive
ER positive
ER negative
Normal HER-2 HER-2 amplified HER-2 amplified
26
Non-luminal
4
Non-malignant
13
Basal/Progenitor
9
Mesenchymal
1 HER-2
Amplified
1 HER-2
Amplified
M
BZR 175
75
CA 30
M
A
M -1
B1
HC 34
UA C2
CC 02
-8
9
EF 3
M
SU 19
M
EF 190
M
19
M 2A
BHC 36
C1 1
HC 50
C1 0
41
HC 9
C
M 38
BM 415
CF
U A -1 0
CC A
HC -81
C2 2
2
ZR 18
M
DA 75M 1
B4
5
18 3
4A
1
T4
7D
M
CF
7
B
M
T
DA -2
M 0
B4
3
BT 5
47
SK 4
BR
KP 3
HC L1
M C1
DA 14
3
M
B
HC 23
C1 1
SU 395
M
-2
HS 25
57
8
18 T
UA 4B
CC 5
7
CA 32
L5
BT 1
CO 54
LO 9
DU 824
4
HC 47
C1 5
HC 18
C1 7
HC 56
C1 9
HC 80
C 6
HC 193
C1 7
95
HC 4
C
M 70
B43
M 6
M
B1
DA 5
M 7
B4
68
PD-0332991: CDK 4/6 Inhibitor: Breast Panel
1000
900
800
700
600
500
400
300
200
100
0
Subtype
Luminal
HER2 Amplified
Immortalized
Non-luminal/post EMT
Non-luminal
PD 0332991: Cell Cycle Analysis
MCF7
%
E FM192A
H C C 1419
100
100
100
90
90
90
80
80
80
70
70
70
60
60
60
50
50
50
40
40
40
30
30
30
20
20
20
10
10
10
0
0
G 0/G 1
S
G2
0
G 0/G 1
S
G2
G 0/G 1
S
G2
Sensitive lines
H C C 1937
%
H C C 1187
MD A MB 468
100
100
100
90
90
90
80
80
80
70
70
70
60
60
60
50
50
50
40
40
40
30
30
30
20
20
20
10
10
10
0
0
G 0/G 1
S
G2
0
G 0/G 1
S
Resistant lines
Finn RS, et al. Breast Cancer Res. 2009;11:R77.
G2
G 0/G 1
S
G2
PD 0332991: Effects on Phosphorylation
on Retinoblasoma Gene Product
A. Total pRb
Time
0
30’
60’
12 hr
24 hr
B. Phospho-Rb (serine 780)
48 hr
0
30’
60’
12 hr 24 hr 48 hr
MCF7
MB453
Sensitive
T47D
EFM19
HCC1187
HCC1954
CAL 51
Finn RS, et al. Breast Cancer Res. 2009;11:R77.
Resistant
Hypothesis: Patient Selection in Breast
Cancer Population
Elevated
Cyclin D1
RB
Decreased
p16
Gauthier ML, et al. Cancer Cell. 2007;12:479-491.
100
2
60
CI
MCF7
% Inhibition
80
1
40
20
0
0
Tam
PD
10000
100
5000
2500
50
1250
25
625
12.5
6.25
1000
5000
2500
1250
625
312.5
100
50
25
12.5
6.25
3.125
312
3.125
Concentration (nM)
Concentration (nM)
2
100
60
CI
EFM19
% Inhibition
80
1
40
20
0
0
Tam
PD
5000
2500
50
25
1250
625
312
12.5
Concentration (nM)
6.25
3.125
Tam
5000
2500
PD
50
25
1250
625
312
12.5
6.25
3.125
Concentration (nM)
100
2
Combo
PD-2991
Tamoxifen
60
CI
% Inhibition
80
T47D
1
40
20
0
Tam
PD
5000
2500
1250
625
312
50
25
12.5
Concentration (nM)
6.25
3.125
0
Tam
5000
2500
1250
625
312
PD
50
25
12.5
6.25
3.125
Concentration (nM)
TRIO 18/A5481003: Phase I/II Study of Letrozole in
Combinations With PD-0332991 in Postmenopausal ER+
Advanced Breast Cancer
Phase I complete
Randomized phase II accruing
ClincailTrials.gov. NCT00721409.
TRIO 18: Phase I Patient Summary
Slamon DJ, et al. ASCO 2010. Abstract 3060.
TRIO 18: Most Common AEs (N = 12)
PT, n
Grade 1
Grade 2
Grade 3
Grade 4
Total
Neutropenia
0
1
7
2
10
Fatigue
6
2
0
0
8
Leukopenia
0
3
2
1
6
Nausea
5
0
0
0
5
Diarrhea
4
0
0
0
4
Anemia
2
1
0
0
3
Cough
2
1
0
0
3
Decreased appetite
3
0
0
0
3
Dyspnea
3
0
0
0
3
Hot flush
2
1
0
0
3
Nasal congestion
2
1
0
0
3
Arthralgia
1
1
0
0
2
Back pain
2
0
0
0
2
Creatinine increased
0
1
1
0
2
Slamon DJ, et al. ASCO 2010. Abstract 3060.
TRIO 18: Most Common TreatmentRelated AEs (N = 12)
PT, n
Grade 1
Grade 2
Grade 3
Grade 4
Total
Neutropenia
0
1
7
2
10
Fatigue
4
2
0
0
6
Leukopenia
0
3
2
1
6
Nausea
5
0
0
0
5
Anemia
2
1
0
0
3
Decreased appetite
3
0
0
0
3
Diarrhea
3
0
0
0
3
Hot flush
2
1
0
0
3
Dyspnea
2
0
0
0
2
Headache
1
1
0
0
2
Thrombocytopenia
1
1
0
0
2
Slamon DJ, et al. ASCO 2010. Abstract 3060.
TRIO 18: Phase I Summary
Phase I (N = 12)
• MTD: PD 0332991 125 mg QD (schedule 3/1) in combination with
letrozole 2.5 mg QD
• 3 DLTs:
– 2 patients with grade 4 neutropenia
– 1 patient with 5 doses held due to elevated creatinine deemed treatment related
• No treatment-related SAEs
• No discontinuations due to AEs
– Common treatment-related AEs: neutropenia, leukopenia, fatigue
• No febrile neutropenia
• No drug-drug interaction
• Efficacy: 3 PRs and 9 SDs (PR: 33%; CBR: 67%)
• Median duration of treatment: 12 mos (range: 2-21+)
• Currently 6 patients active
Slamon DJ, et al. ASCO 2010. Abstract 3060.
Hypothesis: Biomarkers Predictive of
PD 0332991 Sensitivity
Desired biomarker profile:
ER+, HER2– Wild-type Rb1
– Plus
• Amplified cyclin D1/CCND1
OR
• Inactivated CDKN2A/p16INK4a
Finn RS, et al. Breast Cancer Res. 2009;11:R77.
Phase II Study Design (Part I, Completed)
ER+, HER2- breast
cancer
Stratification Factors:
Disease site
− Visceral vs bone only
vs other
Disease-free interval
− > 12 vs ≤ 12 mos
R
A
N
D
O
M
I
Z
A
T
I
O
N
N = 60
Primary endpoint: PFS
ClincailTrials.gov. NCT00721409.
Arm A
PD 0332991 125 mg/day
(Schedule 3/1)
+
Letrozole 2.5 mg/day
1:1
Arm B
Letrozole 2.5 mg/day
Phase II Study Design (Part II, Ongoing)
ER+, HER2- breast
cancer
Biomarker Selection
CCND1 amp
And/or loss of p16
R
A
N
D
O
M
I
Z
A
T
I
O
N
N = 150
Primary endpoint: PFS
ClincailTrials.gov. NCT00721409.
Arm A
PD 0332991 125 mg/day
(Schedule 3/1)
+
Letrozole 2.5 mg/day
1:1
Arm B
Letrozole 2.5 mg/day
Similar Observations in Other Histologies
Ovarian cancer[1]
Glioblastoma[2,3]
Multiple myeloma[4]
1. Konecny GE, et al. Clin Cancer Res. 2011;17:1591-1602. 2. Michaud K. Cancer Res. 2010;70:32283238. 3. Wiedemeyer WR, et al. Proc Natl Acad Sci U S A. 2010;107:11501-11506. 4. Menu E, et al.
Cancer Res. 2008;68:5519-5523.
Telomerase and Cancer
Telomerase: reverse transcriptase that adds DNA repeats
(TTAGGG) to the 3’ end of DNA strands (telomere region)
– Consists of 2 molecules each of telomerase reverse transcriptase
(TERT), telomerase RNA (TERC), and dyskerin (DKC1)
Protects DNA from genomic damage/loss during replication
In cancer, cells that lose telomeres become unstable, accumulate
genetic damage, and eventually undergo apoptosis
Activation of telomerase can prevent the apoptosis event and
cause cells to become immortalized
– Telomerase is activated in 90% of cancer (but not somatic cells)
Hypotheses: block telomerase, induce telomere shortening,
genetic instability and cell death
Shay JW, et al. Human Mol Gen. 2001;10:677-685.
Telomerase MOA
Harley Nat rev Cancer 2008
Telomerase and Cancer
Various potential methods of silencing telomerase
– Oligonucleotides
• Target the template region (activation site) of telomerase
• Imetelstat (GRN163L): 13 mer oligonucleotide, not antisense but a
direct telomerase inhibitor[1]
– Vaccines
• Dendritic cell–based (GRNVAC1)
• Use hTERT pulsed autologous dendritic cells
• Phase I: generally well tolerated, achieved levels felt to be
sufficient for hTERT inactivation[2]
• Phase II study in AML as consolidation
• Nondendritic based
• Phase I in solid tumors (V934/V935)[4]
• GV1001 peptide with temozolomide for melanoma[5]
1. Herbert BS, et al. Oncogene. 2005;24:5262-5268. 2. Su Z, et al. J Immunol. 2005;174:3798-3807. 3. ClinicalTrials.gov. NCT00510133.
4. ClinicalTrials.gov. NCT00753415. 5. ClinicalTrials.gov. NCT01247623.
Conclusions
Newer targets in molecular oncology include the CDK pathway
and telomerase
Ongoing clinical studies (TRIO18) with PD 0332991, an oral,
small molecule kinase inhibitor, in breast cancer aim at validating
laboratory science that identified ER+ breast cancer as being
susceptible to CDK 4/6 inhibition
To date, predictable and manageable toxicity has been seen with this
class of agent
Studies with other CDK targeted agents and Cyclin targeted
agents are ongoing
MCL should be “proof of concept”
Telomerase inhibitors are moving to the clinic and hold promise
but predictors of response will be necessary for successful
clinical development
Including vaccine strategies and short-oligos
 0
0