Potassium_disorders
advertisement

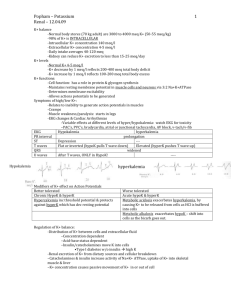
Potassium Disorders Jerry Hladik, MD UNC-Chapel Hill Case 1 A 62 year old male presents to the emergency room with a 2 day history of weakness. His recent history is significant for gouty arthritis for which he was taking over the counter ibuprofen. 140 106 76 100 7.8 15 10 Normal Values 140 104 10 4 24 1 100 Case 2 A 56 year old female presents with a 2 day history of weakness. On physical exam she is diffusely weak and is unable to sit up. The blood pressure is 210/105 mmHg. There is no edema. 140 96 20 1.9 32 1.4 100 140 104 10 100 4 24 1 Normal values Outline • Potassium distribution in the ECF and ICF and factors that alter K distribution. • Renal tubular potassium regulation and excretion • Differential diagnosis of hyperkalemia and hypokalemia Physiologic Effects of Potassium • Major determinant of the resting membrane potential • Hypokalemia – may precipitate cardiac arrhythmias • Hyperkalemia – life threatening cardiac conduction disturbances and arrhythmias Transcellular K+ Distribution 3Na+ ATPase 2K+ K+cell = 140-160 mEq/L K+e = 4-5 mEq/L Relationship Between [K+]serum and Total Body Potassium in 70 kg Adult 6 5 Serum 4 [K+] mEq/L 3 2 -150 mEq Normal +150 mEq Total Body Potassium Potassium Distribution ECF 2% 80 mEq ICF 98% 3920 mEq Potassium Content in Fruits and Vegetables Potato with skin 3 Oz. Dried Fruit 10 Dried Prunes 1 Banana Tomato 1 Kiwi 8 Oz. Glass of Orange Juice 1Grapefruit Amount of Potassium Milligrams mEq 844 mg 20 796 mg 20 626 mg 16 451 mg 11 254 mg 6.5 252 mg 6.5 250 mg 6.5 158 mg 4 A 24 y.o male returns home to visit his mother. For breakfast she serves orange juice (of which he drinks 3 large glasses), and a bowel of fruit comprised of 2 bananas, 1 grapefruit, and 1 kiwi. What would happen to the serum potassium concentration if all of the ingested potassium remained in the extracellular space? Ingested Potassium = 52 mEq Extracellular Potassium = 80 + 52 = 132 mEq Serum K Concentration = 132 mEq/15 L = 8.8 mEq/L ! Components of Potassium Homeostasis ICF Distribution Insulin Intake ECF 90% Kidney Excretion Aldosterone 10% Colon Renal Tubular Potassium Handling Filtered load 600-700 mEq per day K+ Reabsorption 20-30% K+ Secretion K+ Reabsorption 60-70% Urinary Excretion 90mEq/day Urinary Potassium Excretion • Normal kidneys have the capacity to excrete 500600 mEq per day (average K+ excretion 40-100 mEq/day). • The key site of renal potassium excretion regulation occurs at the cortical collecting duct. Cortical Collecting Duct - Principle Cells Na+ Peritubular capillary Na+ 3Na+ ATPase 2K+ Tubular lumen K+ Cl- R-Aldo Aldosterone Cortical Collecting Duct Na+ Tubular lumen Na+ Peritubular Capillary 3Na+ Principle Cell ATPase 2K+ K+ Aldosterone R-Aldo ClH+ ATPase Intercalated Cell NH4+ H+ + NH3 3Na+ ATPase H2O OH- + CO2 K+ T 2K+ HCO3Cl- ATPase H+ NH3 Mechanisms Leading to Hyperkalemia • Impaired entry into cells • Increased release from cells • Decreased urinary excretion Hyperkalemia – Redistribution: ICFECF H+ Glucose Insulin Digoxin β-blockers Cell injury 3Na+ ATPase 2K+ K+ Factors that Impair Urinary K+ Excretion • Collecting duct lumen relatively more electropositive • Decreased flow and sodium delivery to the CCD • Decreased aldosterone production or activity Effect of Amiloride Tubular lumen Predict changes in the following: Peritubular Capillary Amiloride Na+ Channel Amiloride • • • • • Relative lumen charge Renal K+ excretion Serum potassium Renal H+ excretion Arterial pH 3Na+ ATPase 2K+ K+ ATPase H+ 3Na+ ATPase H2O OH- + CO2 Aldosterone R-Aldo T 2K+ HCO3Cl- Hyperkalemia: Decreased Renal Excretion • Volume depletion decreased flow in CCD • Decreased renin-AII-aldo production – – – – NSAIDS renin ACEI AII Heparin aldosterone production Spironolactone aldosterone activity • Inhibition of CCD Na+ channel – Amiloride, triamterene, trimethoprim, pentamidine ECG Changes due to Hyperkalemia ECG Changes of Hyperkalemia Serum K+ (mEq/L) 9 Sinoventricular V-fib 8 Atrial standstill Intraventricular block 7 Tall T wave. Depressed ST segment 6 Tall T wave. Shortened QT interval ECG Effect of i.v. Ca2+ on Membrane Potentials in Hyperkalemia +30 0 i.v. Calcium - 30 -60 Et Em Em Et Et -90 Em Normal K+e K+e Treatment of Hyperkalemia Therapy Mechanism of Action Calcium Stabilization of Membrane Potential Insulin Beta-2 Agonists Bicarbonate Increased K+ entry into Cells Dialysis Cation Exchange Resin (sodium polystyrene = Kayexalate) Potassium removal (if pHa<7.2 in setting of acidosis) Differential Diagnosis of Hypokalemia • Increased entry into cells • Inadequate intake or GI losses • Urinary losses Hypokalemia: Redistribution: ECFICF Insulin β-2 agonists Alkalosis K+ Barium poisoning Hypokalemic periodic paralysis 3Na+ ATPase 2K+ Factors that Enhance Urinary K+ Excretion • Lumen of CCD more electronegative • Enhanced flow and sodium delivery to the CCD • Increased aldosterone Sites of Action of Diuretics Thiazide Diuretics Loop diuretics Lumen (Defect = Bartter’s) Blood Na+ Cl- Lumen Na+ K+ 2Cl-- Loop diuretics Blood Thiazide diuretics (Defect = Gitelman’s) Interpretation of Urinary K+ in the Setting of Hypokalemia GI Losses or prior Diuretic Therapy Renal K Loss or Current Diuretic Use 24o Urine K < 20 mEq > 30 mEq FeK <6% > 10 % Metabolic Alkalosis in Vomiting 35 Volume Depletion 30 25 20 7.0 5.5 4.0 50 30 10 Generation Phase Early Maintenance Phase Late Maintenance Phase Effect of Gastric Loss of HCl, Na+/H2O (Volume) Tubular lumen Predict changes in the following: Peritubular Capillary Na+ Na+ 3Na+ ATPase 1. Relative lumen charge 2. Renal K+ excretion 3. Serum potassium 4. Renal H+ excretion 5. Arterial pH HCO3- 2K+ K+ ATPase H+ 3Na+ ATPase H2O OH- + CO2 Aldosterone R-Aldo T 2K+ HCO3Cl- Aldosterone 110 100 90 ECF Vol (L) Mean arterial Pressure Aldosterone Escape 21 18 15 20 15 10 Na+ balance 200 0 -200 Days 2 4 6 8 10 12 14 16 18 Urine Na+ and Cl- in the Differential Diagnosis of Metabolic Alkalosis and Hypokalemia Condition Vomiting Alkaline urine Acidic urine Diuretic Drug active Remote use Hyperaldosteronism Urine Electrolytes Na+ Cl(meq/L) >15 <15 <15 <15 >15 <15 >15 <15 >15 >15 Case 2 A 56 year old female presents with a 2 day history of weakness. On physical exam she is diffusely weak and is unable to sit up. The blood pressure is 210/105 mmHg. There is no edema. 140 96 20 1.9 32 1.4 100 140 104 10 100 4 24 1 Normal values Case 2 Continued Urine [Na+] = 75 mEq/L Urine [Cl-] = 100 mEq/L FeK = 20% What is the most likely diagnosis?