Electrolyte Management
advertisement

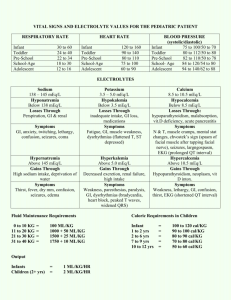
Electrolyte Management Jeff Beamish PGY-3 Intern Bootcamp Lecture Series August 2013 Summary • • • • • • Hyperkalemia Hyponatremia Hypernatremia Hypokalemia Others: Mg, Phos, Ca (briefly only) Cases Disclaimer: this is “boot camp”. I have tried to include the most common issues and management approaches but this lecture was in no way meant to be complete. Hyperkalemia • Life threatening! Hyperkalemia My approach: 1) Is it real? -hemolysis, need to be rechecked? -if there is any uncertainty, get an EKG. 2) How aggressive to do I need to be? -Magnitude: K > 6.0 -Rate of change: K yesterday was 3.5 now is 5.5 -EKG findings: peaked T’s, QRS widening Hyperkalemia Hyperkalemia 3) Appropriate treatment -Ca Gluconate, 1g over 2-3 min -immediate onset -repeat until EKG normalizes -lasts 30-60 min -D50 1-2 amps + 10U IV insulin: -takes 10-30 min to work -lasts 30-60 min -Lasix (if appropriate) -Kayexalate: 15-30 g q6 -slow onset, requires multiple doses to be effective -in 1 day can reduce K by about 1 mEq/dL -DO NOT USE is post operative patients or if SBO suspected -Dialysis 4) Prevent recurrence, figure out etiology: -Renal failure (acute or resulting from missed RRT) -Medications: ACEi, ARB, K sparing diuretics; digoxin; beta-blockers -Acidosis (remember total body K may be depleted) -Tissue damage -etc… Hyponatremia: 1) Do first? or think first? – – Siezures, altered mental status? MICU Otherwise, think… 2) Is it real? Glucose? Other osmotic agents? Lipids? Sorbitol Bladder irrigation? (i.e. what is the likely serum osmolality?) 3) What is the body’s volume status? a) Think: Hypovolemia? CHF? Cirrhosis? Nephrotic syndrome? Other reason why the body might think it is dry? b) check urine osmolarity… Hyponatremia: 4) Fix the problem: • if hypervolemic: – suggested by hypervolemia on exam and/or high urine osmolarity – optimize fluid status (CHF, Cirrhosis, Nephrotic syndrome) • if euvolemic: – – – – Determine etiology: Elevated ADH: SIADH, hypothyroid, adrenal insufficiency Low ADH: beer potomania, polydipsia, tea & toast Medications: HCTZ – Fluid/free water restriction often first line – SIADH note: remember that if the urine osm > than IVF osms, you will make the hyponatremia worse with fluid Hyponatremia: 5) Follow up your management: • Goal correction ~0.5 mEq/L/h • That’s no more than 10-12 mEq/L change per day • Ideally aim for an even slower correction < 9 meq/L per day • Complications most common with very low sodium (< 115) for a long time with rapid correction (>10-12 mEq per day) Hypernatremia: 1) Does this person need ICU? Significant AMS? Seizures? 2) Etiology: • Most commonly hypernatremia for impaired access to free water with ongoing water loss: • Example: Elderly pt with on help at home in a hot apartment with diarrhea • Example: Intubated/sedated on tube feeds at an OSH… • Less commonly from diabetes insipidus • Example: psych patient on lithium • Example: post 40 min cardiac arrest in ICU rewarming • Less commonly from osmotic diuresis: • HHS Workup: check u/a (SG is poor man’s osmolarity) and urine osms. Hypernatremia: 3) Treat: – If possible, give oral free water – Remove offending agents, if possible – If this fails: Hypernatremia: 3) Treat: – If possible, give oral free water – Remove offending agents, if possible – If this fails: • Calculate the free water deficit • Determine the time needed to correct at 0.5 mEq/L/h • Divide free water deficit by time to estimate D5W infusion rate Hypernatremia: 3) Treat: – If possible, give oral free water – Remove offending agents, if possible – If this fails: • The traditional approach involves a simple mass balance on the body and assume essentially no excretion of water or sodium—assumptions that are clearly violated in real life • Does provide a reasonable estimate for starting point: I’ll do some of the calculations for you: All have a Na of 155 and your goal is 145: 50 kg 85 yo woman: 75 cc/h 70 kg 45 yo man: 145 cc/h 120 kg 70 yo man: 211 cc/h Hypernatremia: 3) Treat: – If possible, give oral free water – Remove offending agents, if possible – If this fails: • Much more important: Pick a reasonable starting rate and CHECK YOUR PROGRESS! • Little old lady: 50-75 cc/h • Normal sized guy: 100-125 cc/h • Big guy: 125-175 cc/h Repeat labs every 4-8 h depending on severity. Goal correction LESS THAN 0.5 mEq/h. Pts with DI will need more aggressive volume to meet ongoing losses Hypokalemia My approach: 1) What is the degree of change? (<3 requires immediate attention) 2) What is the Cr? Mg? 3) Is there an etiology for hypoK (that needs to also be corrected if possible)? 1) GI losses: Vomiting, diarrhea, NG suction 2) Renal losses: diuretics, hyperaldosterone 3) Shifts: acidosis, insulin, adrenergic activity Hypokalemia My approach: 4) Replete magnesium (goal > 2 for cardiac patients, 1.5-2 for noncardiac patients—will discuss this in a bit) 5) Replete potassium Normal patient: 10 mEq K increases K by 0.1 mEq/L Maximum K every 4 h is 80 mEq (40 IV, 40 PO) Hypokalemia My approach: (normal renal function, Mg replete) K = 2.8 DANGER 2 Rx: 40 mEq IV now 40 mEq PO q4h x 2 SUBOPTIMAL 3 IV K PO K PO K 40 mEq 40 mEq 40 mEq GOAL 4 Hypokalemia My approach: (normal renal function, Mg replete) K = 3.2 DANGER 2 Rx: 40 mEq IV now 40 mEq PO x 1 --OR-40 mEq PO q4h x 2 SUBOPTIMAL GOAL 4 3 IV K PO K 40 mEq 40 mEq Hypokalemia Other considerations: 1) GFR < 30-40, avoid IV K if possible, give smaller doses, (~50% doses) 2) ESRD, be very cautious (especially if just dialyzed) 1) Supplement only to get out danger zone 2) Use PO K if at all possible 3) Very cautious with IV K, recheck labs frequently 3) Account for ongoing losses 1) Ongoing diarrhea, NG suction 2) Ongoing diuresis (be mindful of overdiuresis can lead to AKI and hyper K) Hypokalemia Special cases: ESRD, just dialyzed last night, AM labs K = 2.8 DANGER 2 Rx: 20-40 mEq PO discuss higher K bath with renal fellow recheck renal panel 6-12 h SUBOPTIMAL 3 PO K 40 mEq GOAL 4 Hypokalemia Special cases: 55 yo woman with HF exacerbation on lasix gtt 10 mEq/h, normal renal function K = 3.0 DANGER 2 Rx: 40 mEq IV, 40 mEq PO q4h x 2 recheck renal panel q12 h, monitor for AKI consider standing K order SUBOPTIMAL 3 GOAL 4 PO IV KK PO K PO K 40 mEq 40 mEq 40 mEq Hypokalemia Special cases: Baseline GFR 30 and stable renal function K = 2.8 DANGER 2 Rx: 40 mEq IV, 40 mEq PO q4h x 1 SUBOPTIMAL 3 IV K PO K 40 mEq 40 mEq GOAL 4 Hypokalemia CHECK YOUR WORK!! 1. Anyone who needs IV K also needs a f/u renal panel at most 12 h later 2. Everyone is different, adjust repletion based on individual responses Others… Hypomagnesemia • • • • Very common You don’t know it’s not there if you don’t look (I usually check a magnesium level on all pt’s I admit at time of admission) Cardiac patients: Mg > 2 mg/dL Toxicity: Mg > 4.8 mg/dl Hypomagnesemia • • Repletion: Slow… Dangerous peak Renal excretion threshold Mg Wasted Mg t Infusion time Mg t Infusion time Hypomagnesemia • • Repletion: normal renal function, goal 2 Very rough guidelines: – – – • • • 1.8-2.0 1 g Mg sulfate / 1h 1.2-1.7 2 g Mg sulfate / 2h < 1.2 4 g Mg sulfate or more over 4h or more If repletion inadequate the next day, try longer infusion time (4g over 12-18 h) Dose with caution in renal failure, GFR < 30, reduce dose by at least 50% Oral: magnesium oxide 200-400 mg BID-TID (causes diarrhea) Hypophosphatemia • • • • Malnutrion, re-feeding syndrome Normal 2.5-4.9 Repletion can be given as sodium or potassium salt IV repletion indicated if Phos < 1.5 – – – – • • • • Choose K-phos (contains 1.5 mmol K for each mol phos) or Na-Phos 2.0-2.5 15 mmol (22 mEq K) 1.0-1.9 21 mmol (31 mEq K) < 1.0 30 mmol (45 mEq K) Often there are shortages: can substitute PO phos, often given every 6 h for a day, then recheck Potassium acid phos tabs have about 4 mEq K / 500 mg Must be infused slowly, cannot be infused with calcium Caution with renal failure. Hypocalcemia 1) 2) 3) 4) Correct for albumin (add 0.8 for each g/dL < 4) Check ionized Ca (need to draw a new sample) Check RFP, Mg, PTH, 25-OH vit D with iCa If IV repletion needed (iCa < 1) • • 5) 6) 0.85-1 2 g Ca Gluconate over 2h < 0.85 3 g Ca Gluconate over 3h Consider etiology Correct underlying problem Again: caution in renal disease (esp with elevated Phos!) Hypercalcemia 1) Correct for albumin (add 0.8 for each g/dL < 4) (it’s probably worse than you think!) 2) Is acute treatment needed (Ca > 12): 1) IV hydration 200-300 cc/h initially then adjust to maintain UOP ~ 100-150 cc/h 2) Lasix AS NEEDED ONLY to maintain euvolemia 3) For Ca > 14: Calcitonin 4 U/kg SQ q6-12h • • 4) Check Ca after 4-6 h and if responding, can continue Rapid tachyphylaxis develops Zolendronate 4 mg IV over 15 min 3) Think about etiology and workup… Cases: 68 yo man evaluated for jaw pain and difficulty eating found to have. CT neck shows LUL spiculated lung lesion: Na = 126 Cl = 87 Cr = 0.71 Ca = 11.2 Alb = 2.7 Now what? Cases: 75 yo man admitted to OSH ICU for hepatic encephalopathy. Admission labs notable for elevated ammonia but otherwise unremarkable. He had been in their MICU for 3 d transferred to the floor at the OSH yesterday and now to you on the VA wards. He remains disoriented and minimally responsive on exam. Na = 159 K = 4.2 Cr = 1.2 Now what? Cases: 56 yo man admitted to ICU after tylenol OD who subsequently develops liver and renal failure, but now transferred to the floor and getting intermittant HD only. Last HD was yesterday. K = 6.0 Now what? Cases: 57 yo man admitted to the VA for Na 121 on routine labs at a CBOC. It took him all day to get to the hospital. You notice he is a little shaky when you meet him. Now what? Cases: 55 yo woman with PMH of extensive CAD s/p recent TAH-SAO for large ovarian mass is admitted to CICU POD # 8 for n/v and CP with transient lateral ST depressions K = 2.8 Now what? Cases: 27 yo woman with h/o of medication nonadherance and DM1 is admitted to UH MICU with DKA. K = 5.8 CO2 = 8, AG 20 BG 423 on arrival What should we do about the K? Cases: 85 yo woman with h/o diastolic HF transferred to Hellerstein service for placement after aggressive diuresis in the CICU. Continues to look wet, but Cr has been rising over the last 3 days from 1.03.0. She is on a lasix gtt at 10 mg/h. 2 days ago her K was 3.0 and now she is getting standing 40 mEq K each evening while on the gtt. K = 5.2 at 4 AM (not hemolyzed) What should we do about the K?