Inflammatory Bowel Disease
advertisement

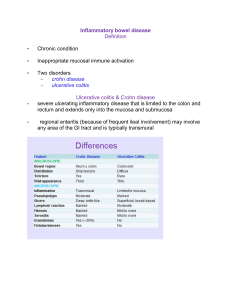
Inflammatory Bowel Disease Overview – Ulcerative colitis and Crohn’s disease are two main forms of IBD, can be differentiated on basis of genetic predisposition, risk factors, and clinical, endoscopic and histologic features – Exact etiology of IBD is unknown, though thought to be related to dysregulated mucosal immune response to commensal gut flora in genetically susceptible individuals Pathophysiology • Exact mechanism for IBD not well understood, though to be related to combination of factors in gut, including: – Damage to epithelial mucin proteins and tight junctions, – Breakdown of homeostatic balance between host’s mucosal immunity and enteric microflora – Genetic polymorphisms in toll-like receptors (TLRs) – Disrupted homeostatic balance between regulatory and effector T-cells Ulcerative colitis Epidemiology • Higher incidence than CD – More commonly seen in North America and Europe • Bimodal incidence pattern – Onset 15-30 years or 50-70s year olds • Genetic factors: Family history very important – Ashkenazi Jews have 3-5x higher risk • Environmental factors – Smoking associated with paradoxically lower risk, milder disease – Hx of prior GI infections, e.g. Shigella, Salmonella, Campylobacter, during adulthood double risk of developing UC, thought to be 2/2 changes in gut flora triggering chronic inflammatory process – Weak associations between NSAIDs, OCPs and increased risk of UC – No data supports psychological stress as trigger for onset or relapse Ulcerative Colitis Clinical Presentation • Common presenting symptoms include rectal bleeding, diarrhea, urgency, tenesmus, abdominal pain – More rarely can see fistulas, weight loss, more common in CD – In severe or advanced cases, patients may present with fever • • Clinical course characterized by alternating periods of remission and relapse Montreal classification used to categorize extent and severity of disease – – – – – E1 (proctitis): inflammation limited to the rectum E2 (left-sided; distal): inflammation limited to the splenic flexure E3 (pancolitis): inflammation extends to the proximal splenic flexure S0 (remission): no symptoms S1 (mild): four or less stools per day (with or without blood), absence of systemic symptoms, normal inflammatory markers – S2 (moderate): four stools per day, minimum signs of systemic symptoms – S3 (severe): six or more bloods per day, pulse rate of ≥90 beats per min, temperature ≥37·5°C, ESR >30 • Extraintestinal manifestations are more commonly seen in UC than CD – include aphthous oral ulcers, iritis/uveitis/episcleritis, seronegative arthritis, ankylosing spondylitis, sacroiliitis, erythema nodosum, pyoderma gangreosum, autoimmune hemolytic anemias and primary sclerosing cholangitis Ulcerative Colitis Diagnosis • Based on clinical symptoms confirmed by objective findings from endoscopic and histologic examinations • Initial w/u must r/o infectious and non-infectious causes of diarrhea • Endoscopic features – loss of vascular pattern, erythema, granular and friable mucosa, erosions, ulcerations and spontaneous bleedings • Pathologic features – distortion of crypt architecture, crypt abscess, infiltration of lamina propria w/ plasma cells, eosinophils, lymphocytes, lymphoid aggregates and mucin depletion Ulcerative Colitis Treatment • Treatment should be tailored to disease activity and extent of disease activity – 5-ASA drugs: E.g. mesalazine, sulfasalazine – Corticosteroids – Immunosuppresants: E.g. azathioprine, 5mercaptopurine – Biologics: E.g. infliximab, adalimumab Ulcerative Colitis Treatment • Surgical treatment required in approximately 2030% of patients. Surgery is generally curative in UC. – Emergency: Life-threatening complications related to fulminant disease unresponsive to medical treatment – Urgent: Severe disease admitted to hospital and not responding to intensive medical treatment – Elective: Refractory disease intolerant to long-term maintenance treatments or colorectal cancer. Ulcerative Colitis Prevention/Screening • UC patients at increased risk of colorectal cancer – 2% after 10 years, 8% after 20 years and 18% after 30 years • Screening colonoscopy beginning at 8 years after disease onset • Following initial colonoscopy, subsequent screening depends on extent of disease – Proctitis/proctosigmoditis: Follow specific age guidelines for surveillance of colorectal cancer – Left-sided colitis/pancolitis: Every 1-2 years – UC w/ PSC: Annually from time of dx of PSC • Risk factors for CRC – Duration and extent of disease – Endoscopic and histologic severity of inflammation Crohn’s Disease Epidemiology • Genetic factors – Family hx well established as one of the strongest risk factors for development for CD • Environmental factors – Lifestyle factors such as tobacco use, sedentary lifestyle, exposure to air pollution, and consumption of western diet • Infectious factors – CD often occurs after infectious gastroenteritis Crohn’s Disease Clinical Presentation • Unlike in UC, Crohn’s disease can affect any portion of the GI tract • Common presenting symptoms – abdominal pain, bloody or watery diarrhea, incontinence, fistulas and perianal symptoms. Extracolonic GI involvement associated with aphthous ulcers, dysphagia, upper abdominal pain and vomiting. • Patients with CD may have hx of other autoimmune disorders, • Montreal classification used to categorize CD – L-classification: Defines extent of disease • • • • • L1: Disease confined to terminal ileum L2: Disease confined to clon L3: Disease involving ileum and colon L4: Disease involving upper GI tract L4+L3: Disease involving upper GI tract and distal disease – B-classification: Defines phenotype • • • • B1: Without stricture formation, non-penetrating B2: Stricturing B3: Penetrating B3p: Perinally penetrating Crohn’s Disease Diagnosis • Clinical diagnosis based on H&P findings with objective findings from history and laboratory studies • As with UC, must r/o important non-infectious causes (IBS, Behcet’s syndrome) and infectious causes (Yersinia, enteroviruses etc.) that mimic CD • Endoscopy is gold standard for diagnosis • Radiologic tests may assist in diagnosis – CT/MRI enterography or enteroclysis – Abdominal U/S • Biomarkers can also be used – CRP, lactoferrin and calprotectin Crohn’s Disease Treatment • All patients with CD should be counseled to quit smoking • As with UC, initial medical treatment depends on phenotype, disease activity, comorbidities and other individual characteristics of patient – In most cases, short course of antibotics, steroids, or anti-TNF agent, e.g. infliximab, adalimumab, combined with thiopurines or methotrexate for long-term maintenance – 5-ASA derivatives, which are mainstay of UC, have shown to be less useful in treatment of CD • Superiority of combination of thiopurines and TNF blockers • No current consensus on optimal length of therapy • Unlike in UC, surgery is not curative in CD Crohn’s Disease Prevention/Screening • Regular screen for active infection – tuberculosis, infections hepatitis, CMV, HIV and C. difficile • Colorectal cancer screening – In patients with more than a third of colon affected (Montreal classification L3), first screening colonoscopy should occur 8 years after onset, repeated every 1-2 years once remission achieved, and every 1-3 years once normal. – Patients with PSC should undergo annual screenings References • Ordás I1, Eckmann L, Talamini M, et al. Ulcerative colitis Lancet. 2012 Nov 3;380(9853):1606-19. • Baumgart DC1, Sandborn WJ. Crohn's disease. Lancet. 2012 Nov 3;380(9853):1590-605.