Inflammation: Osteoarthritis, Crohn's, Appendicitis, Rhinitis
advertisement

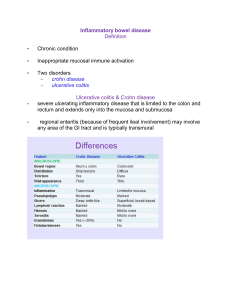
1 Level 3: NMNC 2310 Class Participation Assignment (CPA) CPA #3 Inflammation 1. Explain the difference between Osteoarthritis (OA) and Rheumatoid Arthritis (RA). Discuss clinical manifestations and treatment. In general primary and secondary OA have a higher potential to be inherited, whereas RA’s chances of being inherited are lower in comparison. OA patients experience more wear and tear of cartilage versus the autoimmune component of RA that likes to start with attacking the lining of joints. Typically people over the age of 40 are impacted by OA, in RA there is a higher rate in people near the age of 20. Extra-articular manifestations are not present in OA like RA. There can be an elevation of ESR, CPR, and anti-CCP whereas RA does not see a change in these areas. In order to treat RA immune suppressants are a must, these same drugs are not needed for OA. 2. Differentiate between the treatments for acute cholecystitis and those indicated for cholelithiasis. For acute and mild cases the treatment is non-invasive and more comfort oriented. Patients with acute cholecystitis will have iv therapy (sometimes with corrective electrolytes), iv antibiotics, analgesics and bowel rest. For cholelithiasis things have to come out that is either in the form of removing the whole gallbladder or removing the stones via medication like Ursodiol. 3. What is the difference between Crohn’s Disease and Ulcerative Colitis? Discuss pathophysiology, clinical manifestations and treatment. 2 How Crohn’s disease starts is fairly unknown it is thought that heredity and the immune system are involved, while ulcerative colitis is triggered by a mistake made by the immune system. Inflammation and abscesses progress to aphthoid ulcers which deepen with progression of Chron’s, this inflammation eventually leads to the cobblestoned look associated with Chron’s disease. With ulcerative colitis inflammation of the mucosa and sub-mucosa of the colon and rectum lining develop. When the ulceration has progressed enough it is possible to see the distinction between affected and normal tissue. Because no single treatment works for Crohn’s bowel rest, medicine and surgery are used to treat it. Ulcerative colitis treatment includes medication or surgery. There is no cure for either ulcerative colitis or Crohn’s. 4. Appendicitis can develop in patients across the lifespan. Describe the nursing care for a child with uncomplicated appendix. Describe the clinical manifestations of appendicitis that the child will present with and list nursing interventions and expected patient outcomes after surgery. For this pediatric patient the pain would typically start near the belly button before traveling to the lower right quadrant. Other symptoms that would manifest are a low-grade fever with loss of appetite, nausea and vomiting. The troubles start when the appendix becomes occluded or kinked by a foreign body, fecalith or a tumor. Inflammation causes an increase in intraluminal pressure, from this pressure is the progression to severe pain which can be generalized or near the umbilicus. Eventually (normally a few hours) the pain becomes localized within the lower right quadrant. If the appendix is left alone with its inflammation it will fill with pus and rupture. 3 The child would need to be prepped for surgery to receive an appendectomy. In this scenario peritonitis will not spread, so septicemia is not an immanent threat. Post-op the patient will still have an IV for fluid replacement IV antibiotics may be given too along with placing the patient in a high-fowler’s position so tension can be reduced around the abdominal organs and incision to reduce pain. When the patient is able to handle oral fluids they will be administered. The patient will most likely experience abdominal pain, nausea (from anesthesia), a slight alteration to mental status (e.g. grogginess) on top of becoming a fall risk for a bit. In rare instances the patient may be combative from the anesthesia. 5. You are taking care of a patient who complains of sneezing, itchy skin, watery eyes, clear nasal drainage and nasal congestion. They physician diagnosis the patient with allergic rhinitis. What medications do you anticipate administering to the patient? What patient teaching will you discuss with the patient? Depending on how bad the itching was there might be orders for a topical corticosteroid (e.g. hydrocortisone) with an aerosolized corticosteroid (e.g. fluticasone propionate) if the patient was complaining of facial pain or tenderness. An antihistamine tablet like cetirizine or loratadine maybe given, or an aerosolized Azelastine HCL could be given too (just one, not all three). The aerosolized medications would work faster in terms of relief so if I had to pick it would be those two listed above. For both Fluticasone and Azelastine the patient could do 2 sprays in each nostril once a day, or they could do 1 spray in each nostril two times a day (morning and evening). My instructions would be 4 dependent on their memory and willingness to do something. I would also advise that both medications cap out at 4 sprays in each nostril during a 24 hour period. The patient returns to your clinical two weeks later. The patient is now complaining of facial pain, green nasal drainage, congestion and fatigue. You anticipate that the patient will be diagnosed with sinusitis. What medications do you plan on administering and what patient education can you provide? For the past 6-7 years the go to medication for sinusitis seems to be Augmentin, or at least the doctors I have seen for it like it. I am unsure if this is because of drug reps going into the clinic or if they want to be extra cautious by choosing the pharmacological equivalent of nuking the infection from space. Z-Pak might also be another medication that could be administered. Because the patient came back with worsening symptoms you are also concerned the patient is at risk for Gas Exchange problems. Which Gas Exchange exemplars are you concerned the patient could develop and what preventative teaching can you provide? The exemplars I would be worried about would be dependent on the patient’s medical history, age, allergies, what they did for work and where they lived. A lot of what is under the exemplar list are pretty extreme and need quite a few things to go wrong. An asthma flare up, another bacterial infection like pneumonia, another infection but viral like respiratory syncytial virus, and adult respiratory distress syndrome. Acute respiratory failure is pretty extreme as is infant respiratory distress syndrome, but could happen if everything that could go wrong did go wrong. Teaching wise I would stress the 5 importance of hand washing after blowing their nose or coughing. I would also advise sleeping at an elevated angle would also help. Drinking fluids, resting, and avoiding dairy would also be on my list for patient teaching. Cough drops with menthol would be in my suggestions if they were coughing. If they could tolerate spicy food I would mention that this can give temporary relief sometimes. Speaking from personal experience … I think at this point I would also ask if they were using something like a neti pot daily as using one every day could aggravate a sinus infection or provide a better breeding ground for one in the sinus cavity. I would also ask them to abstain from alcohol as this could dry up their mucosal membranes.