Inflammatory Bowel Disease: Pathophysiology, Diagnosis & Management
advertisement

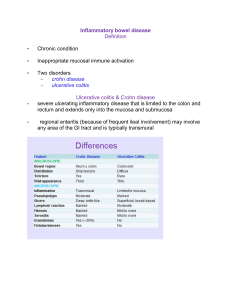
2 Abstract The prevalence of inflammatory conditions that affect the gastrointestinal tract is increasing in adults and children. A greater number of predispositions to such diseases have been identified that include specific environmental factors, which have been associated with its development. This paper explores the pathophysiology of inflammatory bowel diseases including ulcerative colitis and Crohn’s disease. In addition, this piece will provide helpful information regarding the various techniques utilized to assess, diagnose, and manage these conditions. In discussing the above mentioned, the objective of this paper is to provide a helpful guide for the reader to better understand the various etiologies, complications, and approaches to care for inflammatory bowel diseases such as ulcerative colitis and Crohn’s disease. 3 Pathophysiology Ulcerative colitis is defined as a condition characterized by the inflammation and ulceration within the lining of the rectum and gradually up the bowel towards the cecum. Crohn’s disease is best described as when inflammation and ulceration occurs in the lining of any area of the GI tract. Causes of these conditions currently are unknown but there are many risk factors observed in clients with ulcerative colitis to take significant note of. Typical risk factors include infectious agents, autoimmune reactions, allergies, heredity, and foreign objects (Linton & Matteson, 2020). Recent research shows that this disease occurs as an intestinal immune response when there is a predisposed genetic host and specific intraluminal microbiota or other toxic pathogens present (Hindryckx et al., 2016). Although there is no definitive cause for the disease, research continues to focus on the genetic markers observed in clients that have been diagnosed with ulcerative colitis in order to gain better understanding and medical management. Assessment When assessing a patient with ulcerative colitis and Crohn’s disease, it is essential to identify the symptoms for which the patient decided to seek care for. Cardinal symptoms are pain and diarrhea. If the condition includes portions of the stomach and the duodenum, symptoms such as vomiting and epigastric pain are to be expected. If the small intestines are involved in the given condition, then pain, abdominal tenderness, and cramping are expected findings when conducting an assessment (Linton & Matteson, 2020). Upon gathering the presenting symptoms, the nurse should then record the onset, location, severity, and duration of the experienced symptoms. It is important to inquire with the patient what factors may contribute to their symptoms as well as what relieves them such as diet, stressors, and other activities. Note any 4 occurrence of diarrhea, as well as the presence of blood. Lastly the nurse should assess the vitals, the perianal area for irritation or ulceration, intake and output records, as well as the number of stools the patient normally has. In collecting these assessment findings, the nurse can better direct the approach to care they will implement when treating the patient. Lab & Diagnostic Test Common tests typically ordered for Crohn’s and colitis include X-rays, blood tests, CT scan, stool tests, imaging tests, colonoscopy, ultrasonography, or tissue biopsies. Oftentimes, an abdominal radiography is done to rule out any obstruction. The patient will swallow a capsule and this will provide a view of the small intestines. Other lab tests following a radiography are blood tests and stool tests. A CBC will show any signs of infection or anemia. Liver function tests will show any liver or bile duct problems. Electrolytes will most likely show low potassium due to diarrhea from IBD. Vitamin B-12 will also be low due to the small intestine not absorbing nutrients from having Crohn's Disease. (Crohn's & Colitis Foundation. (n.d.). Retrieved November 1, 2021). Further testing will be X-rays of the GI tract. X-rays will show any narrowing of the intestines or intestinal blockage. CT scans are usually done to find complications from the disease such as fistulas, intestinal blockages, or abscesses. Additional testing to look further into the abdomen using a small camera would be an endoscopy. Typical endoscopies that could be performed are colonoscopies and upper GI endoscopies. This can help determine the severity of the disease, as well as differentiate between the two diseases or any other types of intestinal conditions. If the doctor decides to obtain a tissue sample of the colon or an area of the GI tract, they will perform a biopsy. A patient diagnosed with Crohn's disease or colitis will need to have 5 routine blood tests to determine the activity of the disease and to see how well medications are working for them. (Nagaich, 2019). Medication & Surgical Management The first line of treatment for ulcerative colitis and Crohn’s disease involves pharmacological therapy. Based on the severity of the disease, the health as a whole, as well as other possibly contributing factors, the doctor will recommend which medication to use (Crohn’s & Colitis Foundation, 2021). A class of medication used to decrease inflammation in the gastrointestinal tract are aminosalicylates. They contain 5-aminosalicylic, and work particularly best in the colon. Some examples of aminosalicylates include sulfasalazine, mesalamine, olsalazine, and balsalazide. Corticosteroids treat moderate to severe ulcerative colitis and Crohn’s Disease. They suppress the immune system as a whole instead rather certain parts of it. Some examples include prednisone, prednisolone, methylprednisolone, and budenoside. Another class of medication used to treat ulcerative colitis and Crohn’s disease are immunodulators. This class of medication works to suppress the body’s immune response so that inflammation doesn’t continue. In addition, immunodulators are used if aminosalicylates and corticosteroids are not effective. Some examples include azathioprine, 6-mercaptopurine, cyclosporine, and tacrolimus (Crohn’s & Colitis Foundation, 2021). In patients where treatment with medication is unsuccessful, surgery may be recommended. Sudden, severe, ulcerative colitis is the main cause of emergency surgery. A proctocolectomy removes the colon and the rectum. The most common surgery is called a proctocolectomy with ill pouch-anal anastomosis (IPAA). This surgical option restores bowel function and lets stool move and exit through the anus. Laparascopic surgical procedures may 6 also be performed in some cases, and are considered to be a more minimally invasive procedure that oftentimes is the surgery of choice (Crohn’s & Colitis Foundation, 2021). Nursing Care Plan Nursing Diagnosis: Fluid volume deficit r/t intestinal inflammation AEB diarrhea Care Plan Priority #1 Assessment Expected Outcome Assess for changes in LOC, restlessness, dark urine, hypotension, pale/moist/clammy skin, tachycardia Patient will maintain therapeutic fluid volume and electrolyte levels AEB stable VS, good skin turgor, moist mucous membranes, and adequate urinary output Interventions Rationale Administer IV fluids per MD order To prevent further dehydration Weigh client daily and monitor I&O To monitor for any lost or gained fluid volume Provide safety precautions why hypotensive (side rails, bed in low position) To prevent injury Evaluation Patient maintains functional fluid volume and electrolyte balance Patient free of injury Nursing Diagnosis: Acute pain r/t intestinal inflammation AEB abdominal pain and cramping Care Plan Priority #2 Assessment Expected Outcome Interventions Rationale Evaluation 7 Assess for s/s of ulcerative colitis such as: diarrhea, abdominal pain, cramping, rectal bleeding/pain, inability to defecate, weight loss, fatigue, fever Patient will verbalize reduced pain. Assess for elevated v/s Assess any guarding or covering of the abdomen by patient Administer IV/analgesics fluids as ordered by the provider To relieve pain Allow bed rest To promote healing and rest Implement alternative therapeutic measures to relieve pain (music, TV, relaxation) To distract the patient from pain Patient expresses relief of pain AEB VSS and pain level 3/10 or lower Nursing Diagnosis: Inadequate nutrition r/t diet AEB poor eating patterns and food choices Care Plan Priority #3 Assessment Assess for excessive weight loss Assess nutritional history Assess blood lab values (albumin, magnesium, potassium, and sodium) Assess food choices and eating patterns Expected Outcome Interventions Rationale Evaluation Patient will verbalize an understanding of how to manage their condition as well as what their diet should be like to avoid further inflammation to their intestinal tract Educate patient on foods/drinks to avoid when on a low fat, low residue, low fiber diet (whole grains, raw vegetables, fruit skin, seeds, carbonated drinks) Reduce potential inflammation of intestinal tract Patient will follow diet plan and Maintain nutritional diet, small frequent meals To maintain adequate nutrition Patient will maintain adequate nutrition Weigh patient daily To monitor for excessive weight loss Patient’s weight will remain stable 8 References Crohn's & Colitis Foundation. (n.d.). Retrieved November 1, 2021, from https://www.crohnscolitisfoundation.org/. Crohn's & Colitis Foundation. Medication options for ulcerative colitis. (n.d.). Retrieved October 31, 2021, from https://www.crohnscolitisfoundation.org/what-is-ulcerativecolitis/medication. Crohn's & Colitis Foundation. Surgery for ulcerative colitis. (n.d.). Retrieved October 31, 2021, from https://www.crohnscolitisfoundation.org/what-is-ulcerative-colitis/surgery. Hindryckx, P., Jairath, V., & D'haens, G. (2016). Acute severe ulcerative colitis: From pathophysiology to clinical management. Nature Reviews.Gastroenterology & Hepatology, 13(11), 654-664. http://kz21jolix.mp02.y.http.dx.doi.org.proxy.lirn.net/10.1038/ nrgastro.2016.116 Linton, A. D. & Matteson, M. A., (2020). Medical-Surgical Nursing. (7th ed.) Elsevier. Nagaich, N. (2019). Inflammatory bowel disease, ulcerative colitis, Crohn's Disease or indeterminate colitis? Diagnostic Challenge. Gastroenterology: Medicine & Research, 2(4). https://doi.org/10.31031/gmr.2019.02.000545 Veauthier, B. & Hornecker, J. (2018). Crohn’s disease: diagnosis and management. American Family Physician. 98(11), 661-669. https://www.aafp.org/afp/2018/1201/p661.html