INFLAMMATORY BOWEL
DISEASE
Anusha Reddy
FY1 SWFT
3rd Feb 2014
OBJECTIVES
2 Case Studies: Crohn’s Vs Colitis
THINK:
AETIOLOGY
EPIDEMIOLOGY
SIGNS AND SYMPTOMS
INVESTIGATIONS
MANAGEMENT
CASE STUDY 1
22 Female
PC: 6/52 of 5 x loose, non-bloody stools daily
Right lower quadrant abdominal pain (especially
after eating)
8kg weight loss
Bilateral knee and ankle pains
MORE INFORMATION REQUIRED
Full history
Nil PMH, no hx of foreign travel
No medications or allergies
Current smoker- 5 pack-years
Examination
Definite and moderately tender 5-cm mass in the
right lower quadrant
No joint effusion or skin lesions are noted
DIFFERENTIAL DIAGNOSIS
Gastroenteritis
Crohn’s Disease
Ulcerative Colitis
Irritable Bowel Syndrome
Behcet’s Disease
Bowel Cancer
Tuberculosis
Amyloidosis
Acute Appendicitis
WHAT DO WE THINK THIS IS?
22 Female
PC: 6/52 of 5 x loose, non-bloody stools daily
Right lower quadrant abdominal pain (especially
after eating)
8kg weight loss
Bilateral knee and ankle pains
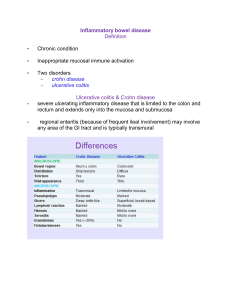
CROHN’S DISEASE- DEFINITION
Chronic Inflammatory Bowel Disease (IBD)
Unknown Aetiology
Characterised by
1.
2.
3.
4.
Focal
Asymmetrical
Transmural
Occasionally granulomatous
inflammation
Any part of the GI tract- mouth anus
CROHN’S DISEASE- EPIDEMIOLOGY
Incidence: 9.56 per 100,0001
Prevalence: 115,000 in the UK
Age of onset: 2 peaks 1) 15-30 Y (more common)
2) 60-80 Y
Female: Male 1.8:1 Children this is reversed!
Risk Factors2
Mycobacterium paratuberculosis, Pseudomonas spp. &
Listeria spp.
↑TNF-alpha
High-fat diets
Genetic mutations
1) Steed H, Walsh S, Reynolds N; Crohn's disease incidence in NHS Tayside. Scott Med J. 2010 Aug;55(3):22-5
2) Rangasamy P et al; Crohn Disease, Medscape, Jun 2011
CROHN’S DISEASE- SYMPTOMS
•
•
•
•
•
•
•
•
•
•
Abdominal pain, cramping or swelling
Anaemia
Fever
Gastrointestinal bleeding
Joint pain
Malabsorption
Persistent or recurrent diarrhoea
Stomach ulcers
Vomiting
Weight loss
CROHN’S DISEASE- ON EXAMINATION
General ill health- weight loss & dehydrated
Hypotension, tachycardia and pyrexia
Abdominal tenderness or distension, palpable
masses.
Anal and perianal lesions (abscesses, fistulae)
Mouth Ulcers
Extra-intestinal manifestations of Crohn’s ......
CROHN’S DISEASE- EXTRA INTESTINAL
INVESTIGATIONS
Bloods
FBC, CRP, U&Es, LFTs
Stool culture and microscopy
anti-S. cerevisiae antibodies Perinuclear
antineutrophil cytoplasmic antibody (p-ANCA)
(UC>CD)
Abdo Xray
Ileocolonscopy and biopsy from the terminal ileum as
well as the affected sites
Small bowel follow through
If upper GI symptoms- Upper GI endoscopy
If lower GI symptoms- Flexible sigmoidoscopy/EUA
CROHN’S DISEASE- MANAGEMENT
1.
First presentation (NICE guidelines)
Glucocorticoids
1.
2.
3.
Prednisolone, Methylprednisolone IV
hydrocortisone
Budesonide
5-ASA
+/- ADD ON Azathioprine or Mercaptopurine
Biologic: Infliximab and Adalimumab
CROHN’S DISEASE- MANAGEMENT
Maintaining Remission (NICE guidelines)
Offer Azathioprine or Mercaptopurine as
Monotherapy
Methotrixate
Surgery- if limited to distal ileum (weighing out
the risk Vs benefits) and for complications...
CROHN’S DISEASE- COMPLICATIONS
B
A
C
C
CASE STUDY 2
32 Male
Bloody diarrhoea 4/52
Bilateral lower abdominal cramping
Malaise and weight loss
No associated fever, visual changes, arthralgias,
or skin lesions
Previously fit and well contractor
Non-smoker, 14-18 units/week drinker
FHx: Diabetes Mellitus Type 1
ULCERATIVE COLITIS- DEFINITION
Chronic Inflammatory
Bowel Disease
Unknown aetiology
Only Large Colon
Classification:
Distal Disease
More extensive disease
Pancolitis
ULCERATIVE COLITIS- EPIDEMIOLOGY
More common than Crohn’s
Incidence: 10 per 100,000
Prevalence 240 per 100,000 in the UK
Age of onset: 2 peaks 1) 15-25 Y (more common)
2) 55-65 Y
Male:Female= 1:1
Idiopathic: ?autoimmune condition triggered by
colonic bacteria inflammation
Genetic component: sibling of an individual who
has IBD 17-35 x more risk of development
Risk of UC decreased in smokers
1) Ulcerative Colitis; NICE Clinical Guideline (Jun 2013)
ULCERATIVE COLITIS- SYMPTOMS
Bloody diarrhoea
Abdominal Pain
Tenesmus
Systemic symptoms: malaise, fever, weightless
ULCERATIVE COLITIS- ON EXAMINATION
Unwell, pale, febrile, dehydrated
Abdo pain and tenderness .. + distension
TOXIC MEGACOLON
Worrying signs: Tachycardia, anaemia and fever
Extra- intestinal disease...
ULCERATIVE COLITIS- EXTRA-INTESTINAL
Aphthous ulcers
Ocular manifestations 5%
Episcleritis
Anterior uveitis
Acute arthropathy affecting the large joints 26%
Sacroiliitis
Ankylosing Spondylitis 3%
Deramatology 19%
Pyoderma gangrenosum
Erythema nodosum
Primary Sclerosing Cholangitis
ULCERATIVE COLITIS- INVESTIGATIONS
Bloods: FBC, LFTs, U+Es, CRP
Serology- pANCA Vs. ASCA
Stool cultures
Imaging
Abdo x-ray- acute setting
Barium enema- can show mucosal structure
Flexible Sigmoidoscopy and Biopsy- for diagnosis
ULCERATIVE COLITIS- MANAGEMENT
a) Topical aminosalicylate
alone (suppository or
enema
b) ?ADD PO
aminosalicylate to a topical
aminosalicylate OR
c) consider an PO
aminosalicylate alone
a) PO Aminosalicylate
- High induction
dose of an
b) ?ADD topical
Aminosalicylate OR
PO beclometasone
dipropionate
- If no improvement 72 hrs
despite IV Hydrocortisone
OR
-Symptoms worsen to
pancolitis:
a) ADD IV Ciclosporin to IV
steroids
ULCERATIVE COLITIS- MANAGEMENT
Indications for Surgery:
Unresponsive to medical treatment
Significantly affecting quality of life
Growth retardation in Children
Life-threatening complications...
Bleeding
Toxic Megacolon
Impending perforation
Carcinoma
ANY QUESTIONS?
SUMMARY
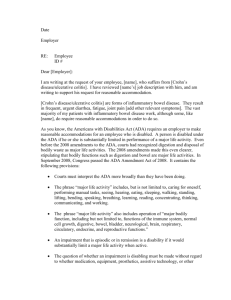
SUMMARY: CROHN’S VS. UC (1)
Symptoms of Crohn's
Disease
Symptoms of Ulcerative
Colitis
• Abdominal pain, cramping or •Bloody diarrhoea
swelling
•Abdominal pain or discomfort
•Anaemia
•Anaemia caused by severe
•Fever
bleeding
•Gastrointestinal bleeding
•Dehydration
•Joint pain
•Fatigue
•Malabsorption
•Fever
•Persistent or recurrent
•Joint pain
diarrhoea
•Loss of appetite
•Stomach ulcers
•Malabsorption
•Vomiting
•Rectal bleeding
•Weight loss
•Urgent bowel movements
•Weight loss
SUMMARY: CROHN’S VS. UC (2)
SUMMARY- CROHN’S VS. UC (3)
SUMMARY: CROHN’S VS. UC (2)
LEARNING POINTS
RELAPSE AND REMITTING
MANAGE THE PATIENT
BONE PROTECTION- IF ON LONG-TERM
STROIDS
TEST FOR TB BEFORE STARTING
INFLIXIMAB
RISK OF COLONIC CARCINIMA IN UC
THANK YOU!!
 0
0