crampy abdominal pain and diarrhea.
advertisement

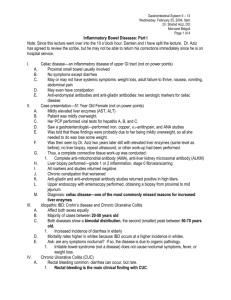
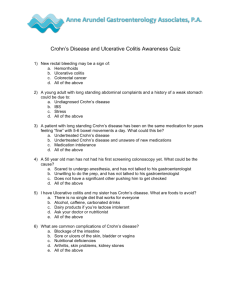
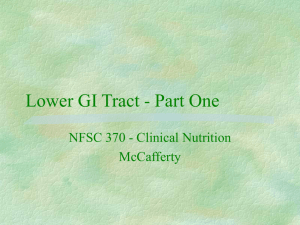
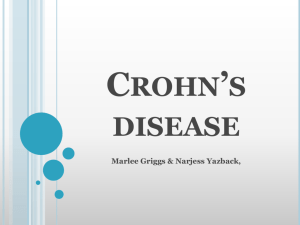
HPI • A 25 year old Caucasian male presents to your clinic with two month history of crampy abdominal pain and diarrhea. • What else would you like to know? HPI continued • Patient also complains of feeling fatigued with an overall lack of energy for the past two months. • He reports a ten pound weight loss since the diarrhea started two months ago. • He has occasionally experienced low grade fevers during this time period. • Patient also reports some achiness in his right shoulder joint and his left knee. This feeling seems to come and go. • Patient denied gross blood seen in stool. Medical History • Past medical history: Exercise-induced asthma • Past surgical history: Tonsillectomy • Family History: Maternal grandmother with “sensitive stomach” • Social History: Smokes half a pack per day, drinks alcohol socially, denies other illicits. Works as a water aerobics instructor. • Medications: Albuterol inhaler prior to exercise • Allergies: Penicillin Patient recap 25 year old male with a two month history of: -diarrhea -crampy abdominal pain -ten pound weight loss -occasional low-grade fever -migratory arthralgias What is on our differential diagnosis?? Differential diagnosis • Irritable bowel syndrome • Lactose intolerance • Inflammatory bowel disease – Crohn’s disease – Ulcerative colitis • Celiac disease • Infectious colitis – – – – Bacterial (ie salmonella) Viral (ie HIV) Fungal (ie histoplasmosis) Parasitic (ie amebiasis) • Neoplastic – Lymphoma – Carcinoid – Etc. What should we do next?? Focused Physical Exam • • • • Vital signs: Temp 98.6 F, BP 122/78, HR 80, RR 18 General: Alert male with slim build. No acute distress. Skin: Pale skin without evidence of rashes. Abdominal exam: – – – – Scaphoid abdomen. Soft with diffuse tenderness upon palpation. Hyperactive bowel sounds appreciated. No organomegaly noted. • Rectal exam: Appropriate sphincter tone. No fissures or abscesses noted. Fecal occult blood test positive. • What tests should we order?? Tests • • • • • • • WBC 12.5 (elevated) Hgb 12.0 (low) ESR 25 mm/hr (elevated) CRP 14 mg/L (elevated) BMP normal Stool tests for ova and parasites negative Would you like any imaging? Colonoscopy Results •Colonoscopy showed areas of inflammation that seemed to skip throughout normal mucosa of the terminal ileum and colon. •Cobblestoning mucosa was also seen, with deep “linear cracks” dispersed throughout the mucosa. •Biopsies were taken and results are seen on the next slide.. Biopsy A biopsy from one of the “skip lesions” shows an infiltration of inflammatory cells interspersed with epilthelioid granulomas, as well as atrophy of the crypts. Resolution • Gastroenterology referral was ordered for treatment of inflammation bowel disease. • The final pathology was consistent with Crohn’s disease. Epidemiology of Crohn’s Disease (CD) • CD is a type of inflammatory bowel disease with a bimodal age of onset. It usually strikes between 15-30 years old, and then between 60-80 years old. • Smoking doubles a person’s risk of developing CD. (Our patient here is a smoker, right?) • It is estimated that around five to ten percent of patients with Crohn’s Disease have a family history of the disease. The remaining majority of patients have no family history. Clinical Presentation • The most common symptoms of CD are abdominal pain and diarrhea. • Fever, weight loss, and fatigue are other common symptoms. • Extraintestinal manifestations can include: – – – – – – Arthritis (most commonly) Eye problems (ie uveitis, iritis) Skin problems (ie erythema nodosum, pyoderma gangrenosum) Renal stones Osteoporosis Vitamin B12 deficiency Histological Characteristics • Macroscopically, CD is characterized by transmural inflammation that can occur anywhere along the GI tract from the mouth to the anus. • From 75-80% of patient have disease involvement in the small intestine- most commonly the terminal ileum. In the picture to the right we see thickened, stenotic colon wall. There are interspersed areas of ulcerations and the cobblestoned appearance is characteristic of CD. Here is a slide displaying a characteristic transmural ulcer in the colon, in which a fissure can now be seen. The fissure is lined by many different cells, including epithelioid histiocytes and giant cells. Above we can see a crypt abscess, which can occur in active CD. The abscess if composed of inflammatory neutrophils. These abscesses often have to be drained under CT guidance if unresponsive to medicine. Additional imaging • Obtaining a CT scan can be helpful to determine the extent disease. •The CT above displays: -Thickening of the terminal ileum wall -Inflammation in the surrounding mesentery •Other possible CT findings with Crohn’s disease include: -Abscesses -Fistulas -Strictures Treatment • Treatment can vary depending on the extent of disease and the symptoms experience by the patient. Below is a list of the range of options available to patients with CD. More in depth discussion of treatment options will occur in third year rotations. • Oral 5-aminosalicylates – i.e. sulfasalazine • Antibiotics – ciprofloxacin, metronidazole • Steroids – i.e. prednisone • Immunomodulators – i.e. azathioprine, methotrexate • Biologics – i.e. infliximab, adalimumab