Abdomen1
advertisement

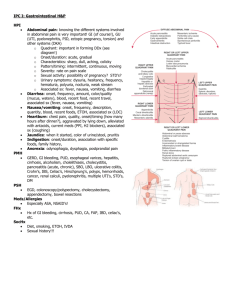
The Abdomen 1. Anatomy & Physiology 2. History 3. Examination & Findings 4. Common Abnormalities The Abdomen Anatomy and Physiology Anatomy and Physiology The Gastrointestinal tract Mouth Esophagus Stomach Small Intestines: Duodenum Jejunum Ileum Large Intestines: Cecum Colon Sigmoid Colon Rectum Anus Function & Control Ingest and Digest Food Absorb Nutrients, Electrolytes and Water Excrete Waste products Controlled by Autonomic Nervous System The Liver Location: right upper quadrant Weight: 3 lbs Composition: four lobes containing lobules, the functional units of the liver Blood supply: hepatic artery brings blood from the aorta directly to the liver. The portal vein brings blood from the digestive tract and the spleen to the liver Three hepatic veins empty blood from the liver into the inferior vena cava Liver Function Metabolism of carbohydrates, fats and protein Glucose is converted and stored as Glycogen Amino acids are broken down and their waste products converted to urea for excretion Amino acids can be converted to glucose: gluconeogenesis Fats arriving as fatty acids are oxidized into carbon components Liver Function Cholesterol is used to form bile salts Storage of vitamins and iron Detoxification, production of antibodies, conjugation & excretion of steroid hormones Production of prothrombin, fibrinogen and other substances for coagulation The liver is responsible for the majority of the proteins circulating in the plasma The Gallbladder Location: under the inferior surface of the liver in the right upper quadrant Function: concentration and storage of bile from the liver Cholecystokinin: a hormone produced by the duodenum: causes bile to be released in the common bile duct and into the duodenum Bile maintains the alkaline pH of the small intestines so fats can be emulsified in order to be absorbed The Pancreas Location: behind and beneath the stomach, epigastric region and left upper quadrant Exocrine function: production of digestive juices containing inactive enzymes for the breakdown of proteins, fats and carbohydrates The pancreatic duct empties into the duodenum, alongside the common bile duct The digestive enzymes become activated in the duodenum The Pancreas Endocrine function: the production of the hormones insulin and glucagon Produced by the islet cells Secreted directly into the blood, to regulate the body’s level of glucose. The Spleen Location: left upper quadrant, above the left kidney, below the diaphragm Composition: lymphoid tissue Function: filter blood as part of the reticuloendothelial system (RES): defense against infection and disposal of products of the breakdown of cells Manufactures lymphocytes and monocytes Storage area for blood Kidneys Posterior View The Kidneys, Ureters, and Bladder Function: reabsorption of electrolytes, small proteins and water, The kidneys control the water and electrolyte balances of the body Elimination of waste products in urine Endocrine Gland: produces renin, important in the control of aldosterone secretion Erythropoietin production:regulates the red blood cell production Production of the active form of vitamin D The Kidneys, Ureters, and Bladder Urine passes into the renal pelvis via the collecting tubules and then into the ureter Peristaltic waves move the urine into a reservoir: the bladder The Bladder has a capacity of 400-500 ml Urine then is eliminated from the body via the urethra The Abdomen History Present Problem Abdominal Pain: Onset and Duration Character Location Associated symptoms: nausea,vomiting, diarrhea, constipation, flatus, belching, jaundice Relationship: body position, inspiration, food intake, menstrual cycle, urination, defecation, time of day Referred Pain Present Problem Indigestion: GERD Character: fullness, heartburn, discomfort, belching, loss of appetite Association: with food intake, time, amount, type of food intake Onset of symptoms: sudden, gradual, day or night Symptom relieve: rest, antacids Medication: OTC and prescribed Nausea: stimuli, with or without vomiting GI Tract Types of Antacids to Look UP OTC (Old Remedy- Tablespoon of Baking Soda) – Alka-Seltzer – Tums – Milk of Magnesia – Pepto-Bismol – Gaviscon – Maalox – Mylanta – Rolaids H2 Histamine Antagonists Axid AR ( Acid Reducer ) Pepcid AC ( Acid Controller ) Tagamet HB ( Heartburn ) Zantac 75 Proton Pump Inhibitors Prevacid 24 HR Prilosec OTC Zegerid OTC Aciphex Odd Man Out Carafate ( Multi-Uses) –Indigestion –Ulcers (peptic and duodenal) –Esophageal Varices Present Problem Vomiting Character: nature, quantity, duration, frequency, ability to keep liquids down Relationship: meals,change in appetite, fever, weight loss Present Problem Diarrhea Character: copious, watery, explosive, color, presence of blood, number of times a day Associated symptoms: chills, fever, thirst, weight loss, pain and or cramping, incontinence Relationship: timing, nature of food intake, stress Travel History Medication: OTC or prescribed, laxatives, stool softeners, antidiarrheals Present Problem Constipation Character: presence of blood: black, bright, tarry. Alternating with diarrhea, with or without abdominal discomfort Pattern: last BM, pain with passage of BM, changes in pattern Diet: recent changes in diet Medication: OTC and prescribed, laxatives, stool softeners, diuretics, iron Present Problem Jaundice Onset and Duration Color of stool and urine Associated with abdominal pain, fever, chills Exposure to Hepatitis Medications: high doses of acetaminophen Past Medical Problem Gastrointestinal Disorders: Peptic Ulcer Disease, GERD, inflammatory Bowel Disease, intestinal Obstruction, Pancreatitis Hepatitis or Cirrhosis of the Liver Surgery: abdominal or urinary tract Major Illness: Cancer, arthritis( steroids/aspirin use), Kidney Disease, Cardiac Disease Blood Transfusions Hepatitis Vaccine Family History Gallbladder Disease Kidney Disease: kidney stones, polycystic disease Malabsorption syndrome: cystic fibrosis, celiac disease Personal and Social History Nutrition: preferences and dislikes, ethnic foods, religious food restrictions, food intolerance's, weight gain or loss Alcohol Intake and use of illegal drugs Recent physical or psychological changes Exposure to infectious disease: flu, travel history Trauma The Abdomen Examination and Findings Epigastric Region 1.Pyloric end of the stomach Duodenum Pancreas Portion of the liver Umbilical Region 2.Omentum Mesentery Transverse Colon Lower part of the Duodenum Jejenum and Ileum Hypogastric Region 3.Ileum Bladder Uterus in pregnancy Right Hypochondriac Region 4.Right lobe of the liver Gallbladder Portion of the Duodenum Hepatic Flexure of the Colon Portion of the right Kidney Suprarenal Gland Left Hypochondric Region 5.Stomach Spleen Tail of the Pancreas Splenic Flexure of the Colon Upper pole of the left Kidney Suprarenal Gland Right Lumbar Region 6.Ascending Colon Lower half of the right Kidney Portion of the Duodenum and Jejunum Left Lumbar Region 7.Descending Colon Lower half of the left Kidney Portion of the Duodenum and Jejunum Right Inguinal Region 8.Cecum Appendix Lower end of Ileum Right Ureter Right Spermatic Cord Right Ovary Left Inguinal Region 9.Sigmoid Colon Left Ureter Left Spermatic Cord Left Ovary Inspection Inspect the abdomen for contour, symmetry and surface motion Note location and contour of umbilicus Distention: above umbilicus: gastric dilation, carcinoma, pancreatic cyst Below umbilicus: ovarian tumor, pregnancy, uterine fibroids, distended bladder Ask patient to take a deep breath on hold it The Fs of Abdominal Distention Fat Fatal Growth Feces Fibroid Flatus Fluid Auscultation Listen for bowelsounds: note frequency and character Borborygmi: stomach growling High-pitched tinkling sounds: suggestive of intestinal fluid and air under pressure, in early obstruction Decreased Bowelsounds: paralytic ileus and with peritonitis Vascular Sounds: listen with the bell for bruits in the aortic, renal ,iliac and femoral arteries Auscultation Auscultation Vascular Sounds Percusion Assessment of size and density of abdominal organs Listen for tympany ( predominant, produced by air in stomach and intestines) and dullness ( over solid organs and masses) Start with an area of tympany and proceed to an area of dullness Percussion Palpation To assess the organs and detect masses, fluid, and areas of tenderness Stand at the right side of the patient in a suspine position, with knees bend for relaxation Make sure your hands are warm Start with a light systematic palpation of all four quadrants Put hand flat on the abdomen and depress the palmar surface of your fingers one cm, use a dipping motion Start away from the pain area Deep Palpation Use the bimanual method One hand for push (Top Hand) , the other hand for feeling (Bottom Hand) Palpation of the Umbilical Ring Palpate around the umbilicus There should be no bulges, nodules or granulation The umbilical ring should be round and regular A soft center or irregularities are suggestive for the potential of an umbilical hernia The umbilicus should not protrude Palpable Structures Palpation of the Liver Place your left hand under the 11th, 12th ribs, fingers pointing toward the head of the patient Press upward to elevate the liver toward the abdominal wall Have patient breath regular a few times then task to take a deep breath Try to feel the edge of the liver against your fingertips as the diaphragm pushes the liver down Liver Palpation Palpation of the Spleen Standing on the right side, reach across and place your left hand beneath the left costovertebral angle Lift the spleen towards the abdominal wall Place your right hand with extended fingers on the patients abdomen below the left costal margin Press your fingertips inward Ask the patient to take a deep breath Try to feel the edge of the spleen as it moves down Palpation Spleen Palpation Spleen Enlarged Liver Common Abnormalities Appendicitis: Epigastric or umbilical pain, later becomes RLQ pain McBurney: rebound tenderness and sharp pain when McBurney point is palpated Associated findings: low grade fever, N / V Cholecystitis: Severe, unrelenting RUQ pain or epigastric pain, may refer to right subscapular area Murphy sign: abrupt stopping of inspiration upon palpation of the gallbladder Common Abnormalities Pancreatitis: Sudden, excruciating LUQ,epigastric pain, may be umbilical. Pain can refer to left shoulder Grey Turner: ecchymosis over flanks Cullen sign; ecchymosis around the umbilicus Associated findings: vomiting, fever, shock Perforated Ulcer: abrupt pain in RUQ, may refer to both shoulders Associated findings: free air and distension with increased resonance over the liver. Tenderness in epigastrium, rigid abdomen Common Abnormalities Diverticulitis: epigastric pain, radiating down the left side of the abdomen, may refer to the back Associated Findings: flatulence, borborygmi, diarrhea, dysuria, tenderness on palpation Intestinal Obstruction: abrupt, severe, spasmodic pain, may refer to epigastrium, umbilicus Associated Findings: distention, vomiting, localized tenderness, visible peristalsis, absent bowelsounds or hyperactive bowelsounds