Medical bedside GIT exam
advertisement

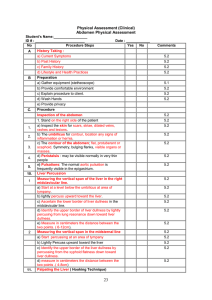
1) Patient should be lying down flat with head on one pillow. Expose patient from the nipple to the pubis. 2) General Inspection Look for a) conscious and alert (hepatic encephalopathy/ uraemic encephalopathy) b) Nutritional status (well built,cachexic,obese) c) Generalised skin pigmentation secondary to -chronic liver disease -haemochromatosis -jaundice if severe. -Wilson’s disease (due to melanin accumulation) d) Pallor e) Observe any urine specimen, any urinary catheter. 3) Hands Look for a) hypoalbuminaemia (leukonychia, Muerchke’s line, Beau’s lines, mees lines) b) Clubbing secondary to either inflammatory bowel disease, celiac disease, liver cirrhosis. c) Koilonychia (iron def.) d) palmar erythema(chronic liver disease) e) Pallor at palmar creases (anemia) f) Dupytren’s contracture (cirrhosis, familial) g) Examine for the presence of liver flap/uraemic flap h) Resting tremors in alcoholics, apparent tremor in Wilson’s disease 4) Upper Limbs Look for a) Signs of bruising, petechiae b) Scratch marks due to pruritus (cholestatic liver disease classically found in primary biliary cirrhosis and can be in uraemia) c) Spider naevi (chronic liver disease) d) Loss of axillary hair (chronic liver disease) e) Muscle wasting 5) Face Look for a) in the eyes - jaundice - pallor - kayser-fleicher rings (Wilson’s disease, cholestatic liver disease) - iritis (circumciliary congestion) inflammatory bowel disease - xanthalesma(primary biliary cirrhosis) - periorbital oedema - periorbital purpura (amyloidosis) - hydration status b) Bilateral parotid gland swelling (found in malnourished alcoholic patients; unilateral parotid gland swelling suggests possible CA or calculus) c) In the mouth and lips - fetor hepaticus - gum hypertrophy (leukaemia, scurvy, gingivitis, phenytoin) - aphthous ulcers (inflammatory bowel disease) - glossitis (iron, folate, B12 deficiency) - angular stomatitis (iron deficiency) - telangiectasia (hereditary haemorhagic telangiectasia) - Pigmentation on the lips,buccal mucosa or palate/circumoral pigmentation (Peutz-Jeghers syndrome) 6) Neck a) Palpate for cervical lymph adenopathy * left supra-clavicular (Virchow’s node) enlargement (Troisier’s sign) Ca Stomach 7) Expose the chest Look for - gynaecomastia - spider naevi(more than 5 is significant) - chest hair loss 8) Examination of the abdomen proper a) Inspection of the abdomen Look for: 1) any distension- causes are fat, flatus(gas), fluid(ascites), faeces, fetus(pregnancy),big tumor(ovarian, fibroid) 2) surgical scars 3) prominent and dilated veins - caput medusae arising from the umbilicus - lateral abdominal veins due to IVC or SVC obstruction 4) Obvious pulsations (AAA) 5) visible peristalsis(could indicate intestinal obstruction) 6) skin- lesions - Sister Joseph’s nodule - Discolorations (Cullen’s sign, Grey turner’s sign) - Striae b) Palpation Superficial, deep Describe: location, size, shape, surface, edge, consistency, tenderness, movement with respiration, pulsatile or non-pulsatile Guarding: voluntary or involuntary. Involuntary guarding: inflammation of the parietal peritoneum. If localized this is normally due to inflammation of an underlying organ e.g. right iliac fossa tenderness could be due to a pathology in the appendix, caecum or right ovary. The liver spleen and the kidneys move on respiration Classical signs to look for - Murphy’s sign (acute cholecystitis) - Rovsing’s sign in acute appendicitis(palpation of the LIF CAUSES PAIN IN RIF) - Iliopsoas sign (appendicitis) 1) LIVER Palpate. The right hand inches towards right costal margin during expiration. During inspiration the liver moves downwards and is felt. Percuss top and bottom. Enlarged liver describe: size, surface, edge, consistency, tender/not tender, pulsatile/not pulsatile and whether there is an audible bruit. The Liver is occasionally palpable in thin individuals. 2) SPLEEN Feel on inspiration. Move hand on expiration. Feel along length of the costal margin as the position of the splenic tip is variable. If not palpable roll patient to right and repeat. This time place left hand over the left lower ribs and attempt to push the ribs towards your right hand. Percuss over the Traube’s area. 3) KIDNEYS Patient inspires. Left hand pushes kidney upwards. Percuss: dull as grossly enlarged kidney displaces the bowels c) Percussion 1) Shifting dullness. Percuss from midline to flank. If there is an area of dullness keep your finger fixed in that position. Roll patient to side. Wait for 30-60 seconds (Talley) then re-percuss. 2) Fluid thrill Present only if there is a huge amount of fluid. Ask the patient to place his right hand over the midline of his abdomen. Place your left hand against the left wall of the abdomen. Use your right fingers to flick the right side of the abdomen. If you feel the impulse in the left hand the fluid thrill is positive. Remember that an enlarged ovarian cyst can elicit a similar response. d) Auscultation. Bell Bowel sounds: right of umbilicus 5-10sec. Absent bowel sounds could indicate paralytic ileus or peritonitis (due to peritonealintestinal reflex). Aortic bruit: above umbilicus Renal bruit: 2 cm laterally 9) Inguinal exam: hernias, swellings 10) Scrotum, testes 11) PR exam Common investigations in GIT diseases 1) Blood Test a. FBE b. ESR c. CRP d. Urea and electrolytes 2) Imaging Test a. X-ray 3) 4) 5) 6) 7) b. Ultrasound c. CT scan d. MRI e. PET scan Barium contrast studies: a. Barium swallow and follow through b. Barium enema c. Double contrast barium enema Endoscopy a. Upper GI endoscope b. Colonoscope c. Sigmoidoscope Endoscopic Retrograde Cholangiopancreatography (ERCP) – both diagnostic and therapeutic Magnetic Resonance Cholangiopancreatography (MRCP) Percutaneous Transhepatic Cholangiography (PTC) Can you name these scars?