here
advertisement

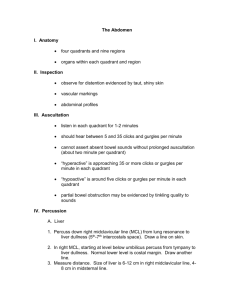
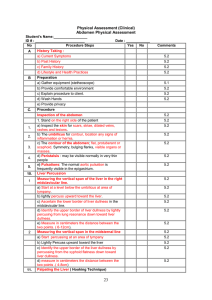
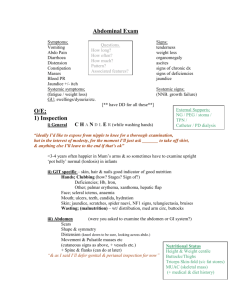
The Abdomen – Chapter 9 Anatomy Notes Divisions: 4 Quadrants (RU, LU, RL, LL) or 9 Divisions --sigmoid colon: often palpable as a narrow firm tube in LL quadrant --cecum/ascending colon: softer palpable tube in RL quadrant --lower margin of liver in RU quadrant (superficial to kidney) --under ribcage/diaphragm: most of liver, stomach, normal spleen --spleen lies against diaphragm at level of ribs 9-11 (posterior to midaxillary line) Diagnostic Notes Pain (Onset, Location, Duration, Character, Aggravating/Relieving, Referred, Timing Visceral (due to forceful contraction or stretch/distension of internal organs) --difficult to localize b/c no direct pain receptors (usually) Qualities: gnawing, burning, cramping, aching Typicals: RUQ: biliary tree and liver Epigastric: stomach, duodenum, pancreas Periumbilical: small intestine, appendix, prox. Colon Suprapubic/Sacral: rectum Hypogastric: colon Parietal (inflammatory process of parietal peritoneum) Quality: severe; aggravated by movement Referred (felt at distant sites w/approximate innervation) Typicals: Duodenal/Pancreatic pain back Biliary tree R shoulder or R posterior chest Pleurisy/Acute MI upper abdomen Examination Inspection Skin (scars, striae, dilated veins, rashes/lesions) Umbilicus Contour of Abdomen (flat, rounded, protuberant, scaphoid; regional/local bulges; visible masses) Movement (peristalsis, pulsations) Auscultation Bowel sounds in all 4 quadrants Bruits (Aorta, Renal aa., Iliac aa., Femoral aa.) Percussion Size/Location estimates (liver, spleen) Liver: 6-12 cm (midclavicular); 4-8 cm (midsternal) Spleen Traube’s space – area b/t lung resonance and costal margin in which the spleen is found Splenic Percussion Sign – percuss lowest interspace in L axillary line; positive sign is a change from tympanic to dull upon deep insipration Gastric/Intestinal fullness Palpation Light and Deep Liver: tenderness on edge during inspiration Spleen: tenderness; only moderately palpable @ inspir. Abdominal Aorta: midline, <3 cm diam. Inflammatory Assess (cough-induced pain, rebound tenderness) Special Techniques Ascites Assessment (suggested by protuberant abdomen w/bulging flanks Palpation: medial tympany w/lateral dullness (margins move when pt changes positions) Fluid wave Appendicitis Hx: pain begins near umbilicus and shits to RLQ (increased by coughing) --localized tenderness in RLQ (or R flank) --suggested when rebound tenderness is present --may present w/cutaneous hyperesthesia (tested by doing skin folds over the abdomen) Rovsing’s Sign – press deeply in LLQ and withdraw quickly (positive is referred pain on pressure or release in RLQ) Psoas sign – while holding down @ knee, ask pt to raise leg (positive is pain) Obturator sign – flex @ hip w/leg bent and internally rotate (positive is R hypogastric pain) Cholecystitis --pain and tenderness in RUQ Murphy’s Sign – hook under costal margin where rectus crosses (positive is increased localized pain/tenderness upon deep inspiration) Abnormality Notes --Heartburn suggests gastric reflux into esophagus (precipitated by heavy meals, lying down, alcohol, acidic foods, aspirin) --possible DDx for regurgitation: esophageal narrowing (stricture/cancer), incompetent LES --hematemesis indicatory of duodenal or peptic ulcer, esophageal or gastric varices, gastritis --RUQ visceral pain indicatory of liver distension (2° to alcoholic hepatitis) --periumbilical visceral pain indicatory of acute appendicitis (transitioning to RLQ parietal pain) --protuberant/tympatic abdomen suggestions intestinal obstruction