Boo-Boo and Owie Repair for Dummies
advertisement

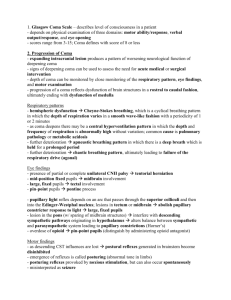
Evaluation of Altered Mental Status Kalpesh Patel, MD Dept. of Pediatric Emergency Medicine October 25, 2006 Objectives To understand the different terms used for level of consciousness. To understand to pathophysiology behind altered level of consciousness (ALOC). To review the differential diagnosis for ALOC. To learn important physical exam findings to clue you into the etiology of ALOC. To review the basic management of ALOC. 2 Definitions Consciousness defined as being awake and aware of both one’s self and one’s surroundings. • Age specific responses Altered Consciousness covers a spectrum of states: • Consciousness • Coma • Lethargy • Confusion/Disorientation • Stupor or Obtunded 3 Definitions Consciousness Confusion/Disorientation – occurs in the order of time, place, person, then unconsciousness Stupor or Obtunded – not totally asleep, but diminished response to external stimuli Lethargy – Depressed consciousness like a deep sleep state where pt roused, but immediately returns to deep sleep Coma – complete unawareness and unresponsiveness States change over time, so pt specific responses are preferable descriptors 4 Epidemiology Bimodal distribution Infection accounts for 1/3 of nontraumatic cases Congenital malformations present in the first few postnatal months DKA more common in adolescence Inborn errors present in infancy Toxic ingestion common in childhood and adolescence Rate of trauma increases throughout childhood 5 Pathogenesis Cerebral hemispheres – cognition, affect, perception of themselves and environment Wakefulness – Ascending Reticular Activating System (ARAS) • Midbrain/pons 6 Pathogenesis Near cranial nerves II, III, VI, and VIII and MLF • Controls pupillary light reflexes and eye movements Impingement of cranial nerves suggests impingement of ARAS Pupillary responses proved the most direct window to the brain 7 Pathophysiolgy Compression of the ARAS usually results from structural causes Diffuse cerebral dysfunction usually has a medical basis 8 Etiologies Altered Level of Consciousness (ALOC): • One of the most difficult diagnostic and management problems in pediatric emergency medicine • Requires quick action to avoid irreversible damage • Wide array of possible diagnoses ALOC is a symptom of another problem, not a diagnosis itself Helpful mnemonic is AEIOU TIPS 9 Etiologies A – Alcohol, Abuse (physical or substance) E – Encephalopathy, Electrolytes I – Insulin, Intussusception, Inborn errors O – Overdose, Oxygen deficiency U - Uremia T – Trauma, Temperature abnormality, Tumor I - Infection P – Poisoning, Psychiatric, Psychogenic S – Shock, Stroke, Seizures, Shunt 10 Herniation Syndromes Increased ICP • Found in many etiologies causing space occupying lesions • Requires immediate identification and action Focal neurologic signs suggest a structural lesion, lack of focality suggests a medical cause • Exceptions: Acute hydrocephalus Bilateral subdural hematomas Acute bilateral cerebrovascular disease Encephalopathies with focal signs Postictal states such as Todd paralysis Beware of Cushing’s triad – hypertension, bradycardia, irregular respirations 11 Herniation Syndromes Central herniation • Pressure in both hemispheres • Pushes midbrain and upper brainstem through tentorium Foramen Magnum (Tonsillar) herniation • Posterior fossa pressure • Pushes cerebellar tonsils through foramen magnum 12 Herniation Syndromes Cingulate gyrus herniation • Unilateral cerebral hemisphere pressure • Pushes gyrus beneath falx cerebri Uncal herniation • Unilateral volume increase • Pushes lower midline cerebrum and hippocampal gyrus through tentorium 13 ALOC Clinical Features 4 pathophysiologic variables are helpful • Respiratory pattern • Pupillary light reflexes • Spontaneous eye movements • Motor responses 14 Respiratory Pattern Ventilation is governed by lower pons and medulla • Modulated by forebrain cortical centers Patterns from rostrocaudal involvement • Post-ventilation apnea lasts 10-30 sec followed by voluntary deep breathing Forebrain involvement • Cheyne Stokes respirations Hyperpnea alternating with apnea Depth of breathing crescendo-decrescendo Diencephalon of deep cerebral hemispheres Caused by failing respiratory center of brain 15 Respiratory Pattern Central neurogenic hyperventilation • Regular and rapid respirations • Normal PaO2 and low PaCO2 • Midbrain • Brain’s attempt to reduce ICP Apneustic breathing • Deep, gasping inspiration with a pause at full inspiration followed by a brief, insufficient release • Signifies damage to Pons/medulla 16 Pupillary Reflex Pupillary pathways near ARAS Pupillary pathways resistant to metabolic insult Single most important physical finding to distinguish structural vs metabolic disease 17 Pupillary Reflex Unequal, sluggish or unreactive pupils (1) Eye is affected is on the side of the lesion (2) Bilateral enlarged and unreactive pupils indicate massive CNS dysfunction (3) Drugs also affect pupils • Opiates – pinpoint pupils • Anticholinergics – large pupils 18 Eye Movements In light stage of coma, roving side-to-side movements occur Persistent deviation to one side may indicate focal seizure activity Structural brainstem lesions abolish conjugate eye movements Oculocephalic reflex (“doll’s eyes”) – hold eyelids open and rotate head from side to side • Normal or positive – conjugate deviation of eyes away from direction of head movement • Contraindicated in c-spine injury • 19 http://prohealthsys.com/physical/movies/cranialnerve_n_13.mov Eye Movements Oculovestibular reflex – elevate head of bed 30 degrees and inject 10-50ml of ice water into ear canal • Normal response is nystagmus with slow phase towards irrigated ear and fast beats away • Unconscious pt with intact brainstem eyes move towards stimulus and remain tonically deviated for a minute and slowly return to midline • Contraindicated if tympanic membrane not intact 20 Eye Movements Cerebral lesions – eyes deviated towards side of lesion Brainstem lesions – eyes deviated away from side of lesion Setting sun sign – downward deviation of eyes • Upper midbrain lesions and hydrocephalus Third nerve paralysis – eyes point down and out • http://cim.ucdavis.edu/EyeRelease/Interface/TopFrame.htm Brief fundoscopic exam should also be performed looking for papilledema or retinal hemorrhages. 21 Motor Responses Assess muscle strength, tone and deep tendon reflexes for normality and symmetry Assess if pt can localize motor responses to determine level of brain lesion • Decerebrate posturing – flexion of upper extremities with extension of lower extremities Lesion in cortex or subcortical white matter 22 Motor Responses Decorticate posturing – rigid extension of arms and legs • Lesion at brainstem, usually pons Flaccid – gravest prognosis with lesion deep in brainstem 23 Management ABC’s with neck immobilization if history of trauma Bedside glucose Hyperventilation to PaCO2 of around 35 mm Hg if increased ICP suspected • Increase ventilation until pupils constrict Support perfusion Neuro exam • GCS or AVPU • Pupillary response • Respiratory pattern • Treat hypoglycemia with glucose or glucagon IM • Consider Naloxone 24 Management Formulate presumptive diagnosis using AEIOU TIPS Pursue specific management Admit to PICU: • Any pt not responding to therapeutic intervention • Require ongoing monitoring • Diagnosis in question after initial management 25 Prognosis In general, pediatric coma patients fare better than adults Predictors of poor outcome • Long (>25 min) duration of cardiac arrest • Blood glucose >250 • Unresponsiveness on arrival • GCS <8 on arrival • pH < 7.10 on presentation • Coma > 24 hours 26 Trauma Epidural Hematoma • Lens shaped • Caused by arterial rupture • Skull fracture present in 85% of cases 27 Trauma 28 Subdural hematoma • Crescent shaped • Caused by tearing of bridging veins through dura and arachnoid • Skull fracture present in 30% of cases • Retinal Hemorrhage in 75% of cases Trauma Cerebral Contusion • Can lead to increased ICP 29 Trauma Cerebral Edema • Loss of gray-white matter interface • Loss of sulci • Occurs 12-24 hours after injury 30 Seizure All seizures except petit mal are followed by a post-ictal state Measure drug levels for children on anticonvulsants Comatose patients may have non-convulsive seizures needing an EEG to diagnose Assume intracranial lesion with non-immediate post traumatic seizure or new focal seizure until proven otherwise Fever- consider meningitis, encephalitis, brain abscess, or febrile seizure 31 Meningitis Bacterial • Most common infection severe enough to cause profound ALOC Non-bacterial • Slower onset of symptoms 32 Infection Brain Abscess • Chronic sinusitis, chronic otitis, dental infection, endocarditis or uncorrected cyanotic congenital heart disease can increase risk 33 Encephalitis Encephalitis – inflammation of the brain parenchyma usually due to viral infection • Mumps and Measles common before immunization • Varicella – occurs 2-9 days after rash develops • Arthropod – varies by geographic areas and seasonal • HSV – most common devastating cause Death or permanent neurologic damage in 70% of cases Affects temporal lobes causing seizures, parenchymal swelling and uncal herniation 34 Tumor Tumors • Can cause seizure, hemorrhage, increased ICP and can invade into ARAS • Ataxia and vomiting, think infratentorial • Seizure, hemiparesis, speech or intellectual problems, think supratentorial • Headache, lethargy, vomiting, think acute hydrocephalus 35 Stroke (Cerebrovascular) Hemorrhagic is usually due to aneurysm • Severe headache • “Sentinal bleeds” are common before rupture • Subarachnoid blood is seen AVM or cavernous hemangioma • Low flow and less acute symptoms 36 Stroke (Cerebrovascular) Thrombosis or Embolic Stroke • Occlusion of anterior, middle or posterior cerebral artery will NOT cause coma • Carotid infarct can cause coma • Infarcts eventually lead to increased ICP • Cerebellar infarcts rarely have coma • Basilar Artery infarcts cause rapid coma due to brainstem damage 37 Shunts Placed for hydrocephalus Malfunction due to mechanical causes or infection Highest risk of failure in first 6 months after surgery Intrathecal baclofen pump overdose can cause coma 38 Hypoxia Neurons extremely sensitive to hypoxia and cease function within seconds of hypoxia Permanent CNS dysfunction can occur within 4-5 minutes of total anoxia at body temperature Hypercarbia can also cause neurologic depression and coma 39 Temperature Hypothermia • Each drop by 1 degree celcius causes a 6% drop in cerebral blood flow • 29-31 degrees – delerium, confusion, muscle rigidity • 25-29 degrees – comatose, no DTR’s, fixed and dialated pupils Hyperthermia • Headache, vomiting, seizure, obtundation, or coma result especially above 41 degrees C • Infants left in a car exposed to sunlight 40 Hypertension May lead to cerebral hemorrhage Hypertensive encephalopathy • Usually due to renal, endocrine or cardiac pathology or toxic ingestion (cocaine) • Headache, N/V, vision changes, ALOC and coma can result • Condition improves once BP has normalized 41 Electrolytes ALOC may be caused by: • Abnormality in any cation (Na, Ca, Mg, Phosphorus) • Metabolic acidosis or alkalosis • Hyperammonemia from inborn errors, urea cycle Hypoglycemia – most common cause in pediatrics • Infants and small children have decreased gluconeogensis • SBI, Sepsis, dehydration, ethanol or oral hypoglycemic ingestion are causes Hyperglycemia – especially new onset diabetes have ALOC due to hyperosmolarity • DKA can lead to cerebral edema 42 Psych Psychiatric disorders can produce stupor like state Psychogenic • Neuro exam reveals this Pt avoids hand falling into face Resists eyelid opening Increased heart rate to painful stimulus Intact neuro exam 43 Other Causes Renal or Hepatic failure Hemolytic Uremic Syndrome can cause coma from uremia or from basal ganglia infarction Reye’s Syndrome • Antecedent viral illness • Mitochondrial injury affects all organs • Severe vomiting followed by combative delirium, then coma • Cerebral edema results leading to central herniation 44 Bibliography Avner, JR. Altered states of consciousness. Pediatrics in Review 2006;9:331-338 Gausche-Hill, M, Fuchs, S, Yamamoto, L. APLS The Pediatric Emergency Medicine Resource Revised Fourth Edition. American Academy of Pediatrics and American College of Emergency Physicians, 2007. p147-153. Fleisher, GR, Ludwig, S, Henretig, FM. Textbook of Pediatric Emergency Medicine Fifth Edition. Lippincott Williams & Wilkins 2006. p201-212. Kanich W, Brady WJ, et al. Altered mental status: evaluation and etiology in the ED. Am J Emerg Med 2002;20:613-617. Meyer PG, Ducrocq S, Carli P. Pediatric neurologic emergencies. Curr Opin Crit Care. 2001;36:651-659. 45