Neurological Assessment
advertisement

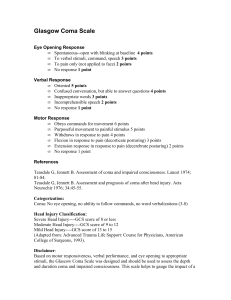
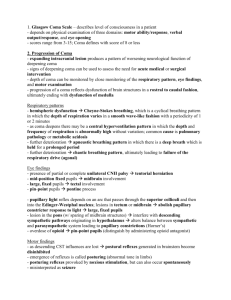
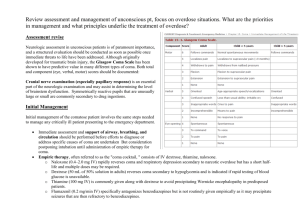
PCA, Glasgow Coma Scale, Canadian Neurological Stroke Scale Patient controlled Analgesia Breaks the pain cycle Gives the control to the patient (often using less narcotic) Avoids peaks and valleys Decreases chance of errors Decreases nursing workload Mechanics of the various systems of PCA RN programs pump according to Dr’s orders in dose increments( 2 nurse check) Minimum interval between doses (lock out period) Client initiates dose by pressing hand held button IV is tkvo or at a regular rate Usually morphine/ fentanyl/ demerol Who is a candidate for PCA? Must need parenteral meds Must have a willingness to operate pump Mentally alert and competent Able to follow instructions who Isn’t Patients with chronic pulmonary disease (predisposition to respiratory depression) History of drug abuse Major psychiatric disorders Children (some) Some elderly etc roles RPN Role: Assessment Documentation (pca assessment and sedation score) Reporting tolerance & changes, + & - RN role: Program pump Ongoing assessment Documentation Maintenance of medication syringes in the pump Assessment Baseline vital signs Ongoing comparison to baseline Allergies Assess pain and sedation level Volume delivered and attempts made Teaching Usually done pre-op so the patient understands how it works Should provide both written and verbal instructions (how to notify staff if inadequate control, change in pain intensity, machine malfunction, alarms Pain Team Usually comprised of and RN/Nurse Practitioner with Pain Management training MD- usually an Anesthetist Neuro assessments -CVA To assess state of neurological impairment & pick up subtle changes 1. Pupillary Response : 2. Mentation: 3. Motor Function: Expressive or Receptive 4. Vital Signs *refer to handouts- Canadian Neurological Stroke Scale and Neurological Observation Record Pupillary response Size Shape Reaction to light Ability to move together Equal bilaterally? Mentation LOC alert/drowsy Orientation oriented/disoriented Speech normal receptive deficit- unable to understand written or spoken words expressive deficit – understands but unable to write or speak effectively Motor Function-Expressive Face Arm Arm Leg Leg -smile -proximal -distal -proximal -distal Motor Function-Receptive Face mimic grin or watch expression with pressure to sternum Arms place arms outstretched @ 90 Legs place thighs toward body Vital Signs Assess resp. watch for cheyne-stokes, rate and rhythm Watch for widening pulse pressure(difference between systolic and diastolic pressure) Can signifiy increased Intrcranial Pressure or ICP Glasgow Coma Scale Assess depth and duration of coma & impaired consciousness Used for acute brain injury D/T: -traumatic injury -vascular injury -infections -metabolic disorders(hypoglycemia, renal failure, ketoacidosis, hepatic failure) Glasgow coma scale Head Injury Classification (GCS) COMA: No eye opening, No ability to follow commands,No word verbalizations Death less than 3 Severe H I 3 to 8 Moderate H I 9 to 12 Mild H I 13 to 15 Normal 15 Learning activities Complete Neurological Stroke Scale on your partner and switch Complete Glasgow Coma Scale on your partner and switch