Global Mental Health: Focus on
Latino Populations
Javier I Escobar MD
Associate Dean for Global Health and
Professor of Psychiatry and Family Medicine,
UMDN-Robert Wood Johnson Medical School
September 2011
Local Health
International
Health
Global
Health
GLOBAL HEALTH
“Health problems, issues, and
concerns transcend national
boundaries, may be influenced by
circumstances or experiences in
other countries, and are best
addressed by cooperative actions
and solutions.”
The Institute of Medicine
US Commitment to Global
Health
• The President asked congress to spend $ 63 billion
over the next six years on a broader Global Health
strategy that would reshape previous policy.
• According to the President, this US global health
investment is an important component of the national
security “smart power strategy”, where the power of
America’s development tools can build the capacity of
government institutions and reduce the risk of conflict
before it gathers strength.
• It has been also recommended that Global Health
should become the pillar of US Foreign Policy*
*Institute of Medicine report released on 12/22/2008
We are in a Global Age
US Medical Schools are developing
programs in Global Health (Harvard,
Johns Hopkins, Michigan, NYU and
many others)
NIH Institutes opening Global Health’s
Offices.
Major Universities require significant
time abroad for undergraduates
(Harvard, Princeton, etc.).
“If you are going to come to Harvard College it would be very good
to have a passport” William Kirby, Dean of the Faculty of Arts and
Sciences (Guardian Unlimited, April 27, 2004)
NIH AND GLOBAL
HEALTH
• The new director of NIH,
Francis Collins, listed Global Health
as one of his top four priorities at
the Institute
• Collins plans to expand research efforts to
include diseases endemic to developing
nations and increase research collaboration
with those countries, to alter the world’s
view of the United States, “by emphasizing
its role as a doctor rather than a soldier”
NIMH INTERNATIONAL ACTIVITIES
In 2004, there were 184 NIMH-funded research
projects that included an international component, only
a handful of these (5 or less) taking place in Latin
America.
By 2009, the director reported that there were 200
projects with an international component.
In 2010, first RFA to create “International Hubs”
(one of them in Latin America)
In 2011, second RFA for “International Hubs”*
*We are submitting application that includes UMDNJ and sites in
Colombia, Mexico, Argentina and Peru.
US Medical Schools and Hospitals
Expanding Overseas
Weill Cornell Medical Center: Cornell Medical
School in Qatar
Duke University: Duke Medical School in Singapore
Johns Hopkins: Two Hospitals in the United Arab
Emirates and one in Singapore
Cleveland Clinic: Hospital in Abu Dhabi
University of Pittsburgh (UPMC): Oncology centers in
Greece, Turkey, Germany, South Korea
Why “Global Health” in Places
Like New Jersey or Zaragoza
Spain?
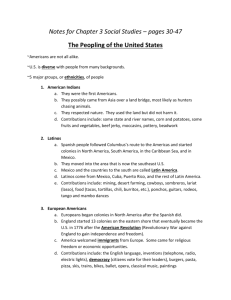
Latinos in New Jersey
400,000
350,000
300,000
250,000
200,000
150,000
100,000
50,000
0
ns ans ans ians ans ans ians rans lans rans
a
c
b
c
ic
ri
b
u
x
o
ni
uv ado ema ndu
Ri
i
m
e
r
d
C
o
M olo
ua
Pe alv uat
re to Dom
H
c
C
S
E
G
Pu
Source : U.S. Census, 2000
Latinos in New Brunswick
48% of all residents
30
25
20
26
23
18
15
10
5
8
7
7
7
3
0
o
n
n
n
a
n
a
a
i
c
c
c
t
i
i
a
Ri
in
er
L
o
m
M
o
er
rt
Am
e
h
D
t
S
O
Pu
C/
n
ci a
ex
Source: New Brunswick Community Health Survey,
Center for State Health Policy, 2004
B
ck
la
W
hi
te
Al
th
O
l
er
Latinos in New Brunswick
Mexican
C/S
American
Dominican
Puerto Rican
Not US
citizen
84%
63%
62%
0
Spanish at
home
99%
87%
94%
51%
Adult
uninsured
70%
51%
39%
23%
Adult MH
(fair/poor)
41%
23%
43%
25%
Anxiety
symptoms
6%
11%
8%
10%
Depression
symptoms
12%
13%
13%
22%
Source: New Brunswick Community Health Survey,
Center for State Health Policy, 2004
Country Origin of Latino Patients
Recruited in a Primary Care Study at
Eric B. Chandler Clinic, in New Brunswick
(Escobar J.I., et al Annals of Family Medicine, 2007)
44%
13%
1.2%
ub
a
1.2%
Pe
ru
12%
C
rg
e
Ri
ca
2.4%
A
C
ra
g
ic
a
N
os
ta
or
ua
4.7%
ad
SA
4.8%
U
ol
om
bi
a
H
on
du
ra
Pu
s
er
to
R
ic
o
ep
.
C
om
.R
D
M
ex
ic
o
5%
nt
in
a
3.5%
8%
Ec
u
9%
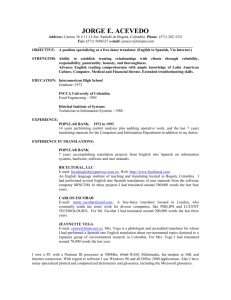
Concentration of Foreign-born Immigrants in Zaragoza
Delicias, Casco Viejo
A. Fullaondo, P. Garcia, www.enhr2007rotterdam.nl
Immigrants in Zaragoza (2006)
Argelia
China
4%
4%
Colombia
7%
Rumania
24%
Marruecos
8%
Ecuador
17%
Otros Varios
36%
Total Population =
660,895
Immigrants =
65,012
Immigrants in Zaragoza, Spain
Zaragoza = the smallest among Spanish Metropolis.
2001 = 14,583 (2%)
2005 = 53,492 (8%)
2006 = 65,012 (10%)
2008 = 92,491 (12%)
2010 = 108,373 (>15%)
Immigrants account for >90 % of the demographic growth in
the city.
More than one fourth of all immigrants come from Ecuador
and Colombia. Other immigrant groups (Asians and other
Europeans) have been on the increase recently.
Most Important Global
Health Problems Nowadays
Communicable, Maternal, Perinatal
and Nutritional Conditions
Non-communicable Diseases
(Chronic Diseases; Mental Disorders)
Injuries
Other (Obesity, Violence, etc.)
LIFE EXPECTANCY AND INCOME
THE WORLDWIDE BURDEN
HISTORY OF EMERGING
INFECTIONS
YEAR
610
644
900
1348
1495
1510
1546
1557
1567
DISEASE
Influenza
Leprosy
Smallpox
Plague
Syphilis
Scarlet Fever
Typhus
Malaria
Smallpox
History of Emerging Infections
1973
1977
1977
1981
1982
1983
1983
1991
1991
1994
1998
1999
2001
2003
2006
Rotavirus
Ebola Virus
Legionnaire’s Disease
Toxic Shock Syndrome
Lyme Disease
HIV-AIDS
Helicobacter Pylori
Multi Drug Resistant
(MDR) TB
Epidemic Cholera
Cryptosporidium
Hong-Kong Bird Flu
West Nile Virus
Anthrax
SARS
Extremely Drug Resistant (XDR) TB)
West Nile Virus in the US
WNV Activity 9/04 T=1386 Deaths 35
AIDS Pandemic
AIDS undoubtedly was one of
the most devastating diseases
that emerged during the 20th century.
o
From 1981 to the end of 2004, about 25
million people world-wide have succumbed
to HIV infections.
o
The pandemic is expected to progress
well into the 21th century.
o
Influenza
An agent of great concern
globally is influenza virus.
Influenza virus is known to cause
epidemics as early as the 1500’s, and
pandemics have been described as early
as 1889.
The most extensive pandemic ever
known is the pandemic of influenza of
1918-1919, which killed more 20 million
people.
Ref Business Week, April 14, 2003
Malaria
Trachoma
Trachoma is an infectious eye
disease. the result of infection
of the eye with Chlamydia trachomatis.
Trachoma is the leading cause
of blindness in the world (Africa, China, Thailand, Mexico,
Brazil, Ecuador).
In the USA = Native Americans and the
Appalachian Region
• Globally, 84 million people suffer from active infection
and nearly 8 million people are visually impaired as a
result of this disease. ...
Trachoma
Infection spreads from person to person,
and is frequently passed from child to child
and from child to mother, especially where
there are shortages of water, numerous
flies, and crowded living conditions.
Infection often begins during infancy or
childhood and can become chronic. If left
untreated, the infection eventually causes
the eyelid to turn inwards, which in turn
causes the eyelashes to rub on the eyeball,
resulting in intense pain and scarring of the
front of the eye. This ultimately leads to
irreversible blindness, typically between
30and 40 years of age.
WHO’s SAFE
Surgery
Antibiotics
Facial Cleansing
Enhanced Hygiene
NCS in the Global Front
• Most people nowadays die from noncommunicable diseases (NCS) once
associated with wealth such as cancer,
heart diseases, diabetes, etc.
• In 2008, 36 million deaths or 63% of all
deaths worldwide, were due to NCS.
• In late September 2011 a high level
summit of the United Nations will be
addressing this problem
Complex Global Health
Problems:
Mental Disorders
Addiction
Obesity
Violence
Injuries
Leading Causes of Disability Around The World
(Cost in Billions of US Dollars)
Schizophrenia
Arthritis
Congenital
Defects
Bipolar
COPD
Alcohol
Falls
Anemia
$0.00
$10.00
$20.00
World Health Organization, 1996
$30.00
Depression
$40.00
$50.00
Obesity
Violence
Addiction
DALYs Lost Due to
High-Risk Drinking by
Disease Category and
Region (2001)
11.8
9.7
Injury
12.0
1.5
Millions of
DALYs
6.8
8.0
3.1
1.5
4.0
6.5
5.3
Chronic Disease
5.6
4.5
10.3
3.7
1.7
1.1
0.5
3.2
2.8
4.5
0.0
Europe/
Central
Asia
Latin
SubAmerica/ Saharan
Caribbean
Africa
E. Asia/
Pacific
South
Asia
Notes: Numbers are rounded.
Source: Disease Control Priorities in Developing Countries, second edition, 2006, Table 47.3
HighIncome
Countries
The WHO ranking of the world’s
health care systems
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
France
Italy
San Marino
Andorra
Malta
Singapore
Spain
Oman
Austria
Japan
Norway
Portugal
Monaco
Greece
Iceland
Luxembourg
Netherlands
United Kingdom
WHO Health Report, 2000
19. Ireland
20. Switzerland
21. Belgium
22.Colombia
23. Sweden
24. Cyprus
25. Germany
26. Saudi Arabia
27. United Arab Emirates
28. Israel
29. Morocco
30. Canada
31. Finland
32. Australia
33.Chile
34. Denmark
35. Dominica
36.United States of America
Total Health Expenditures as %
of GDP, 2002-2005
1. Marshall Islands (19%)
2. USA (>14%)
3. Niue
4. Timor-Leste
5. Micronesia
6. Kiribati
7. Maldives
8. Malawi
9. Switzerland
10. France (10%)
11. Germany (10%)
40.Spain (7-8%)
41. United Kingdom (78%)
60.Colombia (7-8%)
Source = WHO
Disability Adjusted Life
Expectancy at Birth
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
Japan
Australia
France
Sweden
Spain
Italy
Greece
Switzerland
Monaco
Andorra
San Marino
Canada
Source, WHO, 1999
13. Netherlands
14. United Kingdom
15. Norway
16. Belgium
17. Austria
18. Luxembourg
19. Iceland
20. Finland
21. Malta
22. Germany
23. Israel
24. United States of
America
RWJMS Office of Global Health
Located at CAB Suite 7038
o Javier I Escobar MD,
Associate Dean for Global Health
o Aparna Kalbag MD, PhD, Post
Doctoral Fellow
o Rachel Werner, Administrative
Assistant
o Steering Committee:
Sunanda Gaur MD (Pediatrics), Robert Like MD; Sonia
Garcia-Lambauch MD; Karen Lin MD (Family Medicine),
Charletta Ayers MD (OB & Gyn); Abel Moreyra MD
(Medicine/Cardiology), Shannon O’Hearn MS3, Minyoung
Yang MS3, Peter Murr MS-2, Rhea Itoop MS-2, Shazia
Mehmood MS-2
RWJMS Medical
Students’ Interest in
Global Health
o
o
o
21% of RWJMS 2012 Class Were Born Outside
the United States
Over 20 students in the entering class have
participated in international service activities
prior to medical school on four different
continents
Over 1/3 of first year medical students express
interest in having an international experience
during medical school
LATIN AMERICA:
COLOMBIA
--CES Medical School, Medellín
--Universidad de Antioquia, Medellín
--Universidad de los Andes, Bogota
(Dr. Javier I Escobar)
BRAZIL
--Brazil, Cross Cultural project with Pediatrics (Dr. Moorthy);
--Universidad de Sao Paulo (Dr. Pat Williams, Pediatrics)
ARGENTINA
--Universidad de la Plata (Dr. Abel Moreyra Medicine/Cardiology)
--Universidad de Buenos Aires; Departamento de Salud, San Salvador de Jujuy
MEXICO
--Instituto Mexicano de Psiquiatria
--Universidad Popular Autónoma del Estado de Puebla (UPAEP)
--Universidad de Oaxaca
PERU
--Universidad Cayetano Heredia, Lima
COSTA RICA
--International Health Central American Institute Foundation
, San José
ABOUT 50 RWJMS MEDICAL
STUDENTS WENT ABROAD
IN 2008-2009
60% = MS-II
25% = MS-III
15% = MS-IV
COUNTRIES VISITED
ZAMBIA
DOMINICAN REPUBLIC
MYANMAR
COSTA RICA
GHANA
ARGENTINA
SPAIN
CHINA
SOUTH AFRICA
SWITZERLAND
TIBET
INDIA
GUATEMALA
MEXICO
ECUADOR
COLOMBIA
HIMALAYAS/NEPAL
“RWJMS HAS GONE GLOBAL”
OPPORTUNITIES AND
RESOURCES FOR
INTERNATIONAL MENTAL
HEALTH RESEARCH
Collaborations with Latin America:
Javier I Escobar MD
Addiction in the Americas (CICAD - OAS) Collaboration
with Costa Rica, Mexico, Barbados, Uruguay, El Salvador,
Chile, Colombia (UMDNJ-RWJMS as Coordinating Site)
NIMH/CIR/PAHO: Collaboration in Mental Health
Services Research and Education (USA, Canada, Mexico,
Colombia, Chile, Brazil, Peru, Jamaica)
NIMH-Funded Genetic Study: “Bipolar Endophenotypes in
Population Isolates” – UCLA, Colombia, Costa Rica
NIMH R-13 Mentoring Grant
“Critical Research Issues in Latino Mental Health”
Schizophrenia Study in Argentina.
Outcome of Schizophrenia Across
Cultures (WHO Study-- Jablensky et al, 1992)
Best Outcome Worst Outcome
40
20
s
rh
u
Aa
ue
Pr
ag
on
nd
Lo
W
as
hi
ng
to
n
w
co
M
os
al
i
C
n
da
Ib
a
Ag
ra
0
Familial Expressed Emotion and Relapse
of Schizophrenia
• 26 Studies in Several 600
Countries
(England, USA, Spain,
Germany, Eastern
Europe, Japan,
relapsed
did not relapse
500
400
300
Mexico)
• Percent Relapsing:
Low EE -- 22%
High EE -- 50%
200
100
0
Low EE
High EE
AVAILABLE DATA SETS
World Mental Health Surveys
Participating Countries in the
Americas
Country
Brazil
Canada
Colombia
Costa Rica
Mexico
Peru
United States
Sample Size
5,000
30,000
5,000
5,000
5,000
5,000
25,000
52
World Mental Health Surveys
Participating Countries
Legend
Participating countries
Pending countries
No Data
The boundaries and names shown and the designations used on this map do not imply the expression of any
opinion whatsoever on the part of the World Health Organization concerning the legal status of any country,
territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries.
Dotted lines on maps represent approximate border lines for which there may not yet be full agreement.
WHO 2003. All rights reserved
Use of Cannabis and Cocaine in
Several Countries
USA Canada
Mexico
South America
10
8
6
4
2
0
Marihuana
Medina Mora et al, 2005
Cocaine
Asia
HEALTH DISPARITIES
Diagnostic disparities
Let’s remember the old USA/UK Study
inspired by the Schizophrenias that
“were cured just by crossing the
Atlantic” (From the US to England)!
--This led to structured instruments and
diagnoses to diminish bias ---However, diagnostic bias is here to stay!--
UBHC STUDY (N=19,219)
Percent With Serious Mental Illness
(Dementia, Schizophrenia, MDD, Bipolar)
Latinos
Blacks
Whites
50
45
40
35
30
25
20
15
10
5
0
Minsky S, Vega W, Miskimen T, Gara M, Escobar JI, Arch Gen Psychiatry, 60:637-644, 2003
Percent Diagnosed as Schizophrenia
(N=19,219)
Latinos (N=1531)
Blacks (N= 6,475)
Whites (N=10,339
14
12
10
8
6
4
2
0
Minsky S, Vega W, Miskimen T, Gara M, Escobar JI, Arch Gen Psychiatry,
60:637-644, 2003
IMMIGRATION:
ADVANTAGE OR
DISDVANTAGE?
Immigration
About 50% of Latinos in the US are Immigrants
Hispanics born or living in the US appear to be at a
greater risk for mental disorders than counterparts
born or living in their native countries
Stress of trying to integrate into US society, feelings
of alienation and discrimination may increases risk for
some disorders
Longer time of residence in US and younger age at
entry increase risk for immigrants
Protective effects of strong cultural and familial ties
may weaken when living in the US
Longer residence in US and younger age at immigration
increase risk (vulnerable period?)
Vega WA, et al. 1998; Alderete E, et al. 2000
Epidemiological Studies in USA
Ethnic Groups
Study
Immigrants/
USA
Language
Advantages
Immigrants?
White vs Black vs.
Hispanics
NCSR
299/5124
English
YES
Non-Hispanic Whites
NESARC
1541/23,622
English/Spanish
YES
Mexican Origin
ECA
NCS
MAPSS
NESARC
706/538
English/Spanish
YES
319/58
English
YES
1810/1202
English/Spanish
YES
227/2331
English/Spanish
NCS
NESARC
54/16
434/563
English
NLAAS
1630/924
English/Spanish
Puerto Rican
Hispanics
English/Spanish
YES
NO
NO
NO?
12 Month Prevalence of Mood and Addictive
Disorders in Males (Vega et al, 1997)
10
Drugs
Alcohol
Mania
5
Dysthymia
0
Depression
USA
MEXICO
12-month Substance Abuse/Dependence Rate by Nativity,
Age at Time of Entry into US,
and Present Age
Age 0–16 at Entry US
Age 25+ at Entry US
Age 17–24 at Entry US
US born
20
15
% 10
5
0
10
20
30
40
50
60
Age (years)
• U.S. born significantly different (p < 0.001) from each immigrant group
(controlling for sex and present age).
• Immigrants Age 0–16 at Entry US vs Age 17–24 at Entry US significantly
different (p = 0.02) for present age 18–24.
Vega WA, et al. In press
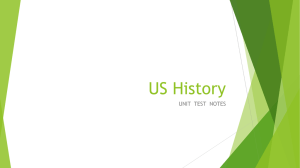
Prevalence of Current Diagnoses in Immigrants and
Native Born in Spain (N=1500 each)*
P<.0001
*Garcia-Campayo et al, 2011
Unhealthy Habits in Pregnant
Women
Positive for Drugs
Positive for Alcohol
45
40
35
30
25
20
15
10
5
0
Latin
White,
Women
US-born
Modified from Vega et al, 1993
Smokers
10 Year Age-Education Adjusted
Coronary Heart Disease Mortality Risk
for Mexican-American Adults
US-born Spanish
US-born English
Mexico-born
30.00%
25.00%
20.00%
15.00%
10.00%
5.00%
0.00%
MALES
FEMALES
Sundquist & Winkleby Am J Public Health, 89:723-730, 1999
Cultural Gradient and
Blood Pressure
Average Systolic Blood Pressure
125
Whites
Latin Immigrants
120
115
110
105
100
95
Low
Middle
Socioeconomic Status
Steffen PR, Journal of Behavioral Medicine, 29: 501-510, 2006
High
Cardiovascular Paradox in
New Jersey
(Moreyra et al, presented at GHEC,
Cuernavaca, Mexico, Abril 2010)
Table 1. Clinical Characteristics
NJ 1994-2007
Hospitalized AMI
Hispanic
n=13,106
Whites
n=190,142
n (%)
6.5%
93.6%
Age, y
67 + 15*
71 + 14
Hypertension, n (%)
69.7%*
63.7%
Diabetes Mellitus, n (%)
39.2%*
29.1%
Renal Disease, n (%)
11.3%*
11.5%
• Hispanics were younger (67 years vs. 71 years),
• more likely to have
– hypertension (70% vs. 64%),
– and diabetes (39% vs. 29%),
• all differences significant, p<0.0001.
Table 2. Multivariable Adjusted Associations
(Interventions)
NJ 1994-2007
Hospitalized AMI
PCI, n (%)
CABG, n (%)
•
•
Hispanic
n=13,106
Whites
n=190,142
Adjusted
OR/HR
(95% CI)
Adjuste
d
p value
21.21%
18.49%
0.94 (0.900.99)
0.03
8.42%
8.81%
0.98 (0.911.07)
0.72
Hispanics had lower adjusted rates of percutaneous interventions:
– (PCI) (OR 0.94, CI 0.90-0.99, p=0.03),
but similar rates of revascularization:
– by CABG (OR 098, CI 0.91-1.07, p=0.72.
Table 2. Multivariable Adjusted Associations
(Mortality)
NJ 1994-2007
Hospitalized AMI
Hispanic
n=13,106
Whites
n=190,142
Adjusted
OR/HR
(95% CI)
Adjuste
d
p value
12%
14.7%
0.88 (0.830.93)
<0.000
1
30 Day Death
13.6%
17.1%
0.95 (0.900.99)
0.047
1 Year Death
22.8%
27.6%
0.98 (0.941.01)
0.23
In-Hospital Death
• Hispanics had lower:
• In-hospital (HR 0.88, CI 0.83-0.93, p<0.001) and
• 30-day mortality (HR 0.95, CI 0.90-0.99, p=0.047),
• But at one year the survival difference was no longer significant
(HR 0.98, CI 0.94-1.01, p=0.23).
Summary of Results
Despite higher prevalence of risk
factors and lower rates of PCI in
Hispanics, the in-hospital and 30day post AMI mortality is lower,
but the difference fades at 1-year.
The Latino Paradox:
Mortality (Hazard Ratios) Latinos vs. Non Latino Whites
in the US (NLMS Data)
1
0.8
0.6
0.4
0.2
0
Males
Mexican
Central/South Amer.
Abraido-Lanza et al AJPH 1999
Females
Puerto Rican
Non-Latino Whites
Cuban
Potential Explanations for Mental
Health “Advantages” of Immigrants in
the US
Measurement Error?
“Salmon” Effect
misinterpretation of questions;
language & translation issues;
Selective Migration
cross-cultural equivalence
Healthier Habits
Kin networks and Family
Response Bias?
social desirability, social
approval, acquiescence
Support?
Advantages of Bilingualism
o
Bilingual people (French/English)
obtain better results in
execution tests, have better
cognitive flexibility, better
ability to negotiate abstract
concepts than monolingual
people1
o
Similar results have been
observed in the case of Hispanic
origin people in the United
States 2,3
1-Peal and Lambert, 1962 2-Rumbaut and Ima 1988 3-Portes 1997)
Immigration and Psychosis:
The Experience in England
o
o
o
o
1960’s: “High prevalence of Schizophrenia
in Caribbean Immigrants to the UK” (1)
1980’s: “Schizophrenia is 14 times higher among Caribbean
immigrants than in the general UK population (2) and this also
applies to the second generation born in England (3)
1990’s: Studies with more methodological sophistication also
showed an excess of schizophrenia (4) and mania (5)
among
Caribbean immigrants. However, other studies showed slight or
no differences (6)
2000’s; The AESOP study calls immigration “a risk factor for
psychosis (7)
1-Sharpley et al, 2001; 2- Harrison et al, 1988; 3-Harrison et al, 1997; 4-Wessely et al,
1991 5- Van Os et al, 1996; 6-Bughra et al 1997; 7- AESOPStudy Group 2002
Social Aspects of the
Caribbean Migration to
the United Kingdom
o
o
o
Disadvantages and travails of Black people and ethnic
minorities in England.
Afro-Caribbeans are more likely to be arrested or be
transported by the police, to be admitted to psychiatric
services against their will and to be locked or confined.
“Diagnoses of psychosis made by White psychiatrists on
Afro-Caribbeans are based on the notion that the
person is strange, undesirable, bizarre, aggressive and
dangerous”
Raleigh and Almond 1995; Fernando 1998; Hickling FW, Robertson-Hickling H,
Hutchinson G, Migration and Mental Health, in Hickling FW, Sorel E (eds), Images of
Psychiatry: The Caribbean, Stephenson Litho Press, Jamaica, 2005 (pages 153-177
Comments on Studies Associating
Psychosis with Migration
o
o
o
o
o
There is ethnic variation in the presentation of psychotic
symptoms 1
Documented bias in the diagnosis pf certain ethnic
groups (African Americans in USA) 2
The diagnosis of Afro-Caribbeans in England is possibly
due to a similar bias.
Studies of Afro-Caribbeans in Jamaica do not show an
excess of psychotic disorders. 3
The results of the old north American studies and the
more recent European studies relating migration and
psychosis may be due to these biases.
1-Vega WA, Lewis-Fernandez R, Current Psychiatric Reports, 2008, 10:223-228
2-Minsky S, Vega W, Miskimen T et al, Arch Gen Psychiatry, 2003, 60:637-644
3-Hickling FW, Sorel E (eds), Images of Psychiatry: The Caribbean, Stephenson Litho Press, Jamaica, 2005
Reflexions on Immigration
and Psychopathology
o
o
o
o
o
o
o
Immigration is a risk factor with a high level of variability.
It is related to motivations for migrating, social conditions,
language, culture, acceptance of the immigrant in the new
environment, employment, etc.
Unfortunately, color of the skin continues to play a
significant role (racism).
Language is a critical factor
Resilience, personality, social support, are protective
factors.
Immigration may have an impact on certain psychiatric
disorders but not in others.
Epidemiological vs. Clinical Studies.