Consultation for National STI Management Guidelines
advertisement

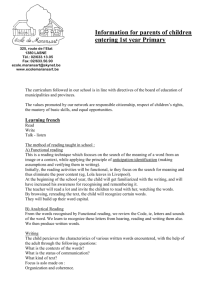
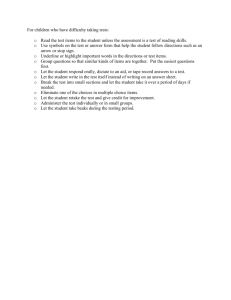
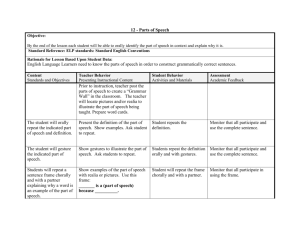
National STI Management Guidelines of Pakistan The National AIDS Control Programme The Provincial AIDS Control Programmes The World Health Organization Basic Outline and Concepts Worldwide epidemiology of STIs • 340 Million new infections annually • Burden unevenly shared more by developing countries • Account for app 17% of health expenses* • HIV is an STI • HIV-STI co-infections (with HSV-2, H. ducreyi) *World Bank. World Development Report: Investing in Health. 1993 Common Terms Used • Provider and clinician are used interchangeably • This can under some circumstances include non doctor providers Epidemiology in Pakistan of STIs • Very common among high risk groups • Moderately common among bridge groups • Uncommon among general population Care seeking for STIs in Pakistan • Similar to other care in Pakistan: >70% in the private sector • Different providers see different types of clients • Syphilis testing and Tx is uncommon • Partner management is rare • Condom promotion is uncommon Counseling and condom promotion • Condoms are the best prevention measure • Counseling works • Patient-provider interactions are the best condom and risk behavior counseling opportunities • Free condom provision • Discussing STI risk behaviors Partner Management • Patient>Partner>Patient reinfection cycle • Patient delivered medicines • More important to focus on the patient’s regular partner Referrals • Difficult STIs • HPV/ warts • Decide or pre-identify whom to refer to • Role of the provincial AIDS Programs The 4 Cs Compliance, Counseling, Condoms and Contact (Partner) Management 4 Cs: Compliance STI patients must be encouraged to comply with their prescribed treatment • Instruct all patients to complete the full course of treatment • Disappearance of symptoms during treatment does not mean that the patient is cured, full course of treatment must be completed • Without proper treatment, STIs may cause severe complications • Patient should avoid sexual contact during the treatment and until partner has been treated • Ensure a follow-up visit 4 Cs: Counseling for Prevention Every patient presenting with STI symptoms must receive and understand education messages tailored for each patient regarding: • STIs result from Sexual contact • Information about safer sex practices and use of condom • The mode of transmission of STIs, including HIV • STI augments the risk of HIV transmission • Offer HIV voluntary counseling and testing (VCT) • Consider syphilis testing 4 Cs: Condom Use To minimize the further transmission of STIs, including HIV, it is essential to educate all clients on the proper use of condoms: • Demonstrate to each patient how to use a condom correctly • Clinic should supply condoms to STI patients 4 Cs: Contact (Partner) Management Patients must understand the importance of partner management even if he/she is asymptomatic: • Risk of re-infection from asymptomatic partner • Risk of complications for his/her partner • Possible ways of partner management include: • Providing additional treatment regimens for the partner • Encouraging partners to come to the clinic for treatment Reproductive Health Linkages Two forms of linkages were identified in our consultations 1. Gynecologists should act as the specialist to whom either difficult infections or patients with warts are sent to 2. All patients that are considered for STI management in gynecology set up must be considered for syphilis testing and if positive for treatment. 3. All patients presenting for STIs are sexually active. This is also an opportunity to discuss family planning and if the method used is condoms, they will provide dual protection (against STIs and from pregnancy) Risk Assessment of patients • Some persons are at more risk of STIs than others due to: – Their behaviors – Where they live • STI algorithms (those for women) work better with high risk patients What is Syndromic Management • History-Exam-Lab paradigm • History-Exam paradigm • Limited laboratory support in most areas • Limited utility of labs when available Benefits of Syndromic Approach • Standardization of care • Cost effectiveness Limitations of the Syndromic Approach • Works better for male STIs • No algorithms for anal symptoms • Female algorithms work better in high risk settings • Syphilis management which requires testing is not well addressed by these guidelines Syndromes discussed 1. 2. 3. 4. 5. 6. Urethral Discharge Genital Ulcer Scrotal Swelling Vaginal Discharge Lower abdominal pain Anal symptoms STIs of interest 1. 2. Human Immunodeficiency Virus (HIV)§ Neisseria gonorrhoeae (NG or GC – short for GonoCocci) 3. Chlamydia trachomatis (CT) 4. Herpes simplex (HSV) (HSV-2) 5. Trichomonas vaginalis (TV) 6. Candida albicans 7. Bacterial Vaginosis (BV)1 8. Syphilis (Treponema pallidum) 9. Human Papilloma Virus (HPV) 10. Haemophilus ducreyi (Chancroid)2 11. Lymphogranuloma Venereum (LGV)2 1. Not actually an STI, included here as it causes symptoms in women 2. Uncommon in Pakistan and therefore will not be addressed in any depth Basic Etiology (causative organisms) of Syndromes Syndrome Urethral discharge Symptoms • Urethral discharge • Dysuria • Frequent urination Signs Most common causes • Urethral discharge • Gonorrhoea • Chlamydia Genital ulcer • Genital sore • Genital ulcer • Syphilis • Chancroid • Genital herpes Scrotal swelling • Scrotal pain and swelling • Scrotal swelling • Gonorrhoea • Chlamydia • Lower abdominal pain • Dyspareunia • • • • • Gonorrhoea • Chlamydia • Mixed anaerobes Lower abdominal pain Vaginal discharge Anal Symptoms • • • • Unusual vaginal discharge Vaginal itching Dysuria (pain on urination) Dyspareunia (pain during sexual intercourse) • Anal Pain • Anal Discharge • Anal or peri-anal sores Vaginal discharge Lower abdominal tenderness on palpation Temperature >38° • Abnormal vaginal • discharge VAGINITIS: • Trichomoniasis • Candidiasis CERVICITIS: • Gonorrhoea • Chlamydia • Anal tenderness • Anal Discharge • Anal or peri-anal Ulcers • Gonorrhoea • Chlamydia • HSV-2 Issues of antibiotic resistance • Empiric prescription of antibiotics • Gonococcal resistance already a problem • Syndromic approach can help or aggravate the problem Evidence Behind the Guidelines Urethral Discharge: • Senstivity 87-99% • Labs seldom add to sensitivity • Labs slightly enhance specificity for CT but not NG Evidence Behind the Guidelines Genital Ulcer: • Senstivity: 72-100% • More sensitive and specific for HSV and Syphilis • Labs add very little to specificity Evidence Behind the Guidelines Vaginal Discharge: • Senstivity: 73-93% when applied to women presenting for STI care • Senstivity: 29-86% when applied to all women screened for STIs • Only 10% of low risk women actually have an STI • Speculum does not add very much to the reliability of the algorithm (sens: ~30, spec: ~50) Common Issues • Protect yourself, wear gloves Syphilitic chancre of fingers Common Issues • Protect yourself, wear gloves • STIs require contact between 2 individuals, think of the partner • Prevent future problems: promote condoms • Counseling when possible (remember the 4 Cs) Referral • Surgical Evaluations are usually emergent • Pre-determine possible providers in your area whom you will refer to • Provincial AIDS Program recommends this provider for …… Common STIs Gonorrhoea • Causes In men In women Urethritis Cervicitis Proctitis Proctitis Pharyngitis Pharyngitis Urethritis • Major complications: Men: Urethral Strictures • Major complications: Women: PID • Major complications: Disseminated Gonorrhoea Treatment of Gonorrhoea Uncomplicated Anal/ Genital Infection Ciprofloxacin 500 mg orally once only (Ciprofloxacin is contraindicated in pregnancy and for children or adolescents) OR Cefixime 400 mg orally once only OR Ceftriaxone 125 mg intramuscularly (IM) once only OR Spectinomycin 2 gm intramuscularly (IM) once only Disseminated Gonococcal infection Ceftriaxone 1 gm intramuscular or intravenous once daily for 7 days OR Spectinomycin 2 gm intramuscularly twice daily for 7 days Neonatal Ophthalmia Ceftriaxone 50mg/ kg intramuscularly as a single dose OR Kanamycin 25 mg/ kg intramuscularly as a single dose OR Spectinomycin 25 mg/ kg intramuscularly as a single dose Treatment of Chlamydia Uncomplicated Anal/ Genital Infection Doxycycline 100 mg orally twice daily for 7 days (Not to be used for pregnant women, children or adolescents) OR Azithromycin 1 gm orally once only Alternative Regimens Amoxycillin 500 mg orally 3 times a day for 7 days OR Erythromycin 500 mg 4 times a day for 7 days OR Ofloxacin 300 mg orally twice a day for 7 days (Please note that all formulations of Ofloxacin in the market have 200 mg, so 2 capsules or tablets will be required) OR Tetracycline 500 mg orally 4 times a day for 7 days Chlamydia • Usual presentation of Chlamydia are similar to Gonorrhoea • Chlamydia is also asymptomatic in many patients • Common presentations of Chlamydia: In men • Conjunctivitis • Urethritis • Proctitis • Epidydmitis • Prostatitis In women • Conjunctivitis • Cervicitis • Proctitis • Urethritis • Endometritis • Salpingitis Complications of Chlamydia: • Infertility • Ectopic pregnancy • Miscarriage Syphilis • One of the oldest diseases on man • 4 stages: Primary, secondary, late latent and tertiary • Congenital syphilis in children born from infected mothers Primary Syphilis • • • • Early infection Lasts for 1-3 months Lesion is called chancre Occurs at the site of the entry of organism (usually genitalia but can be anywhere) • Multiple chancres can occur • Not possible to accurately distinguish from HSV-2 Primary Syphilis Primary syphilis on finger Secondary Syphilis • At this stage the organisms are multiplying and disseminating in the body • Manifestations can occurs all over the body although most commonly happen in skin • Lesions are macular, maculopapular, papular or pustular • Most commonly on palms and soles • May become a painless, broad, moist, gray white to erythematous highly infectious plaques called condyloma lata • May also cause arteritis Secondary Syphilis Clinical Manifestations of Secondary Syphilis Plaques of Condyloma lata Plaques of Condyloma lata Skin •Rash •Macular •Maculopapular •Papular •Pustular •Condyloma latum •Generalized lymphadenopathy •Pruritus Mouth and throat •Mucous patches •Erosions •Ulcer (aphthous) Genital lesions •Chancre •Chondyloma latum •Mucous patch Constitutional symptoms •Fever of unknown origin •Malaise •Pharyngitis, laryngitis •Anorexia, weight loss, Arthralgias Central nervous system • Asymptomatic • Symptomatic • Headache • Meningismus • Meningitis • Ocular • Diplopia • Decreased vision • Otitic • Tinnitus • Vertigo • Cranial nerve involvement (II– VIII) Renal • Glomerulonephritis • Nephrotic syndrome Gastrointestinal • Hepatitis • Intestinal wall invasion Arthritis, osteitis, and periostitis Late Latent Syphilis • This is the phase when the manifestations of the primary and secondary syphilis are over and yet the patient remains infected • 10-25% of these individuals will go on to develop tertiary syphilis Tertiary Syphilis • This is the late stage • Involvement of CNS, eyes, cardiovascular system in addition to late benign syphilis (gumma) Congenital syphilis • Happens by infection of the baby in utero • Many complications – most are serious • We recommend that this condition must always be referred to specialist care Syphilis Testing • 2 types of tests: Treponemal (VDRL, RPR) and Nontreponemal (FTA-ABS, TPHA) • VDRL/RPR become positive earlier and may turn negative in 3-5 years even when untreated • FTA-ABS/TPHA take 2-3 months to turn positive and remain positive for life • VDRL/RPR turn negative in 1+ year after successful treatment (may be upto 2 years) • These patients will require follow up with the titer of VDRL/RPR • FTA-ABS/TPHA response to treatment is not known Treatment of Syphilis Early Syphilis (Primary, Secondary or Latent of less than 2 years duration) Benzathine Penicillin 2.4 million IU intramuscularly once Alternative Regimen Procaine Benzyl Penicillin 1.2 million IU intramuscularly once daily for 10 days Alternative Regimen (for Penicillin allergic patients and non-pregnant patients) Doxycycline 100 mg orally twice a day for 14 days OR Tetracycline 500 mg orally twice a day for 14 days Alternative Regimen (for Penicillin allergic patients and pregnant patients) Erythromycin 500 mg orally 4 times a day for 14 days Treatment of Syphilis Late Latent Syphilis (Infection of more than 2 years duration) Benzathine Penicillin 2.4 million IU intramuscularly once a week for 2 consecutive weeks Alternative Regimen Procaine Benzyl Penicillin 1.2 million IU intramuscularly once daily for 20 days Alternative Regimen for Penicillin allergic patients and non-pregnant patients Doxycycline 100 mg orally twice a day for 30 days OR Tetracycline 500 mg orally 4 times a day for 30 days Alternative Regimen for Penicillin allergic patients and pregnant patients Erythromycin 500 mg orally 4 times a day for 30 days Treatment of Syphilis Neurosyphilis Aqueous Benzyl Penicillin 2-4 million IU by intravenous injection every 4 hours for 14 days (12-24 millions units a day for 14 days) (Ideally it should be referred for admission) (or should we admit all) OR Procaine Benzyl Penicillin 1.2 million IU intramuscularly once daily plus Probenecid 500 mg orally 4 times a day, both given for 10-14 days (Although this regimen is meant for outpatient therapy, please ensure that the patient will remain compliant with FULL treatment) For Penicillin allergic non-pregnant patients Doxycycline 200 mg orally twice a day for 30 days OR Tetracycline 500 mg orally 4 times a day for 30 days Herpes Simplex type-2 (HSV-2) • Common • Mostly asymptomatic • Manifests as blisters or ulcers and is painful • Treatment protocols divided as: first episodes, recurrent episodes and those requiring suppressive therapy • Treatment suppresses symptoms but does not cure infection Treatment of Herpes Simplex type 2 (HSV-2) Treatment of First Episode: Acyclovir 400 mg 3 times a day for 7 days Treatment of Recurrent Episodes: Acyclovir 400 mg 3 times a day for 5 days Suppressive therapy: Acyclovir 400 mg twice a day continuously Trichomonas Vaginalis • Usually presents as a vaginal discharge and vulvovaginal soreness or irritation • Can also cause Dysuria or dyspareunia (usually severe) and lower abdominal discomfort • Diagnosis is usually clinical Treatment of Trichomonas Vaginalis Metronidazole 2 gm orally once OR Tinidazole 2 gm orally once Alternative regimen (also used for urethral infections) Metronidazole 400 or 500 mg orally twice daily for 7 days OR Tinidazole 500 mg orally twice daily for 7 days Bacterial Vaginosis • • • • Commonest cause of vaginal discharge Not an STI (does not effect males) Represents alteration of the vaginal flora Presents as a smelly discharge in lower vagina and labia • Discharge is grayish, thin, homogenous and contains bubbles Treatment of Bacterial Vaginosis Metronidazole 2 gm orally once OR Clindamycin 2% vaginal cream, 5 gm intravaginally at bedtime for 7 days OR Metronidazole 0.75% gel, 5 gm intravaginally twice daily for 7 days OR Clindamycin 300 mg orally twice daily for 7 days Treatment during Pregnancy First Trimester (only if treatment is imperative): Metronidazole 2 gm orally once 2nd or 3rd trimesters: Metronidazole 200- 250 mg 3 times a day for 7 days Alternative regimen Metronidazole 2 gm orally once OR Clindamycin 300 mg orally twice daily for 7 days OR Metronidazole 0.75% gel, 5 gm intravaginally twice daily for 7 days Candida • Due to overgrowth of candida around labia and surrounding areas • Usually represents alteration of vaginal flora or other causes and not an STI • Diagnosis is clinical • Dysuria • Excoriations (redness with peeling of skin) in the perivaginal area • Shallow, radial, linear ulcerations • Vaginal walls are red • Discharge is thick, sticks to skin and has curds • No smell Treatment of Candida Miconazole or clotrimazole 200 mg intarvaginally daily for 3 days OR Clotrimazole 500 mg intravaginallly once OR Fluconazole 150 mg orally once Alternate Regimen Nystatin 100,000 IU intarvaginally daily for 14 days Venereal Warts • Caused by viruses called the Human Papilloma Virus or HPV • Appear as skin tags • Can be very small (barely visible) to several centimeters • In men they are present around shaft of penis • In women they are present around visible parts of the vagina and clitoris although they can be anywhere on the genitalia • Peri-anal warts are present in those engaging in receptive anal sex and may be inside anal canal • Due to the danger of development of cancer, those treated for warts must be referred to assessment of cancer (Pap smear in women and follow up in men) Treatment for Venereal Warts Treatment is meant for external genitalia and vaginal. Please refer to gynaecologic specialist for cervical warts Consider sending patients with warts for gynaecological evaluation since the causative agent of warts (human papilloma virus) increases the risk of cervical cancer Provider administered: Podophyllin 10-25% in compound of tincture or benzoin. Apply carefully avoiding normal tissue. External genital genitalia should be washed thoroughly in 1-4 hours. Allow the applied medicine to dry before removing speculum. Repeat application weekly as needed. OR Cryotherapy (when available). Repeat after 1-2 weeks as needed OR Self applied by the patient: Podophyllin 0.5% twice daily for 3 days then no treatment for 4 days. Follow this cycle for up to 4 times. STI Syndromes Urethral Discharge • • • • Men mostly but women too Gonorrhoea or Chlamydia or both Emphasize confirming discharge No discharge – other abnormality: appropriate algorithm • No discharge – no abnormality: reassure Clinical case • 25 year old man presents to the clinic, sits down and is uncomfortable discussing his complaints • After some probing he admits some difficulty related to penis and some discomfort during urination • He declines any extramarital sex activity and continues to look uncomfortable Learning point • Many patients will not openly discuss their STI related complaints • Many may not accept extramarital sex • Some may start with vague complaints and come to their STI symptom only when comfortable • Confidence and Rapport building are crucial for good STI history taking • Examination of penis to confirm diagnosis of urethral discharge is important Urethral Discharge Discharge from Urethra Expressing discharge from Urethra TREATMENT OF GONORRHOEA Uncomplicated Anal/ Genital Infection URETHRAL DISCHARGE Ciprofloxacin 500 mg orally once only Yes Patient complains of urethral Discharge or dysuria No Any other genital disease Discharge confirmed? (Ciprofloxacin is contraindicated in pregnancy and for children or adolescents) OR Cefixime 400 mg orally once only OR Ceftriaxone 125 mg IM once only No Take history and examine. Milk urethra if necessary Use appropriate flow chart 4 Cs Ask patient to return in 7 days if symptoms persist OR Spectinomycin 2 gm IM once only Disseminated Gonococcal infection Ceftriaxone 1 gm IM or intravenous once daily for 7 days OR Spectinomycin 2 gm IM twice daily for 7 days TREATMENT OF CHLAMYDIA 4 Cs: 1. Compliance Counseling 2. 3. 4. Promote & provide Condoms Counseling for STI prevention, HIV testing; Educate and Reassure patient Partner (Contact) treatment Yes Treat for Gonorrhoea and Chlamydia • 4 Cs • Ask patient to return in 7 days if symptoms persist Uncomplicated Anal/ Genital Infection Doxycycline 100 mg orally twice daily for 7 days (Not to be used for pregnant women, children or adolescents) OR Azithromycin 1 gm orally once only Alternative Regimens Amoxycillin 500 mg orally 3 times a day for 7 days OR Erythromycin 500 mg 4 times a day for 7 days OR Ofloxacin 400 mg orally twice a day for 7 days OR Tetracycline 500 mg orally 4 times a day for 7 days Persistent or Recurrent Discharge • Definition: Discharges that continue to bother patient after 1 wk or more of appropriate Tx • Significance: – Non-adherence – Resistance (gonorrhoea) – Re-infection – Missed Diagnosis • Re-infection may require probing history about sexual relations • Partner management issues TREATMENT OF GONORRHOEA Uncomplicated Anal/ Genital Infection PERSISTENT URETHRAL DISCHARGE Patient complains of urethral Discharge or dysuria Yes Any other genital disease 4 Cs Ask patient to return in 7 days if symptoms persist No Treat for Trichomonas No Discharge confirmed? 4 Cs: 1.Compliance Counseling 2.Promote & provide Condoms 3.Counseling for STI prevention, HIV testing; Educate and Reassure patient 4.Partner (Contact) treatment Yes Does History confirm reinfection or poor compliance • 4 Cs • Ask patient to return in 7 days if symptoms persist Not better Yes Repeat Urethral Discharge Treatment Ciprofloxacin500 mg orally once only (Ciprofloxacin is contraindicated in pregnancy and for children or adolescents) OR Cefixime 400 mg orally once only OR No Take history and examine. Milk urethra if necessary Use appropriate flow chart Refer for laboratory tests and Specialist Care Ceftriaxone125 mg IM once only OR Spectinomycin2 gm IM once only TREATMENT OF CHLAMYDIA Uncomplicated Anal/ Genital Infection Doxycycline100 mg orally twice daily for 7 days (Not to be used for pregnant women, children or adolescents) OR Azithromycin1 gm orally once only Alternative Regimens Amoxycillin500 mg orally 3 times a day for 7 days OR Erythromycin500 mg 4 times a day for 7 days OR Ofloxacin400 mg orally twice a day for 7 days OR Tetracycline500 mg orally 4 times a day for 7 days TREATMENT OF TRICHOMONAS Metronidazole400 or 500 mg orally twice daily for 7 days OR Tinidazole500 mg orally twice daily for 7 days Genital Ulcers • Confirm with exam • Critical distinction: Ulcer (sore) vs Vesicle (blister) • Clinically impossible to differentiate between syphilis, HSV and chancroid in about ½ of ulcers • Clinically relevant situation: Non healing ulcers vs slow healing ulcers • HIV/HSV co-infection and HIV transmission Clinical Case • 21 y/o man presents with severe pain on penis for 3 days • It is causing difficulty with urination • On exam, there is a single ¼ cm ulcer on the glans penis near the urethral meatus Clinical Case • 21 y/o woman presents with severe pain around vagina for 3 days • It is causing difficulty with urination • On exam, there is a single ¼ cm ulcer near the urethra ___________________________ Note: the ulcer may be on the labia, near or on clitoris/ urethra or any where in the genital area Clinical points • Ulcers range from barely visible to over a centimeter in many of the patients • They may be multiple • Multiple ulcers may not all be together (ie they may be in different parts of the genitalia) • They may occur around the anus • In about half of the cases it is impossible to distinguish between HSV and syphilis Genital Ulcers Vulvar ulcer - HSV Vulvar ulcer – Primary syphilis Genital Ulcers Penile ulcer - HSV Peri-vaginal Primary Herpes Genital Ulcers Penile ulcer – primary syphilis Penile Vesicles - HSV GENITAL ULCERS TREATMENT OF HSV-2 Refer for laboratory testing and Specialist treatment Patient complains of genital ulcer Treatment of First Episode: Acyclovir 400 mg 3 times a day for 7 days Treatment of Recurrent Episodes: Take history and examine Only vesicles present Acyclovir 400 mg 3 times a day for 5 Yes Treat for HSV Test and Treat for syphilis 4 Cs Ask patient to return in 7 days if symptoms persist No Sore or ulcer present Yes Treat for syphilis AND HSV 4 Cs Ask patient to return in 7 days if symptoms persist days No Suppressive therapy: Ulcer(s) improving Acyclovir 400 mg twice a day continuously Yes No Ulcer(s) healed Continue treatment for another 7 days Yes TREATMENT OF SYPHILIS is complicated and detailed. Please refer to separate sheet 4 Cs: 1. Compliance Counseling 2. 3. No 4 Cs Reassure 4. Promote & provide Condoms Counseling for STI prevention, HIV testing; Educate and Reassure patient Partner (Contact) treatment Scrotal Swelling • Critical decision: Infectious or Non-infectious • History important for prior trauma • Examination is important to distinguish rotation, elevation or rotation of testes • Infectious causes are usually GC/ CT • Non-infectious causes are usually surgical • Surgical problems require (usually emergent) referral • Remind patients that scrotal swellings particularly that are due to past trauma may take a long time to resolve…. Clinical Case • 19 y/o man presents with scrotal discomfort • There was a history of difficulty urination and perhaps some urethral discharge about 3 weeks ago • There is a history of penetrative sex with a Hijra in the past several weeks • On exam the left side of scrotum is slightly swollen and slightly tender just under the base of penis Clinical points • It is absolutely essential to distinguish infection from surgical causes of scrotal swelling – when in doubt refer for surgical care TREATMENT OF GONORRHOEA Uncomplicated Anal/ Genital Infection SCROTAL SWELLING Ciprofloxacin 500 mg orally once only (Ciprofloxacin is contraindicated in pregnancy and for children or adolescents) OR Patient complains of Scrotal Swelling No History and examination Swelling/ Pain Confirmed 4 Cs: 1. Compliance Counseling 2. 3. 4. Promote & provide Condoms Counseling for STI prevention, HIV testing; Educate and Reassure patient Partner (Contact) treatment Yes Reassure patient Provide analgesics if needed 4 Cs Testes rotated or elevated or history of trauma Cefixime 400 mg orally once only Treat for Gonorrhoea and Chlamydia OR Ceftriaxone 125 mg IM once only OR Spectinomycin 2 gm IM once only No • 4 Cs • Ask patient to return in 7 days if symptoms persist Disseminated Gonococcal infection Ceftriaxone 1 gm IM or intravenous once daily for 7 days OR Spectinomycin 2 gm IM twice daily for 7 days TREATMENT OF CHLAMYDIA Yes Refer for surgical evaluation Uncomplicated Anal/ Genital Infection Doxycycline 100 mg orally twice daily for 7 days (Not to be used for pregnant women, children or adolescents) OR Azithromycin 1 gm orally once only Alternative Regimens Amoxycillin 500 mg orally 3 times a day for 7 days OR Erythromycin 500 mg 4 times a day for 7 days OR Ofloxacin 400 mg orally twice a day for 7 days OR Tetracycline 500 mg orally 4 times a day for 7 days Anal Symptoms • Main concerns: – – – – – Discharge Ulcers Warts Hemorrhoids Rectal Fissures • Proctoscopy increases diagnosis for most common causes • Warts a concern for future development of cancer • Occasionally HSV can also cause anal discharges, Discharges not responding to GC/CT Tx may be tried on HSV-2 Tx Clinical case • A 29 y/o man presents with anal discomfort for one week • On probing, he admits to occasionally selling anal sex, last being about 2 weeks ago • On exam there is anal ulcers Clinical Case • A 35 y/o married man presents with soiling of underwear for a week • The soiling is foul smelling and has caused embarassment for him at his office • He denies any extramarital sex • After some rapport building he admits to having sex with a male colleague but insists that he (your patient) only penetrated • On exam there is purulent anal discharge Clinical Case • A 36 y/o disshevelled man presents with severe pain during defecation • After rapport building he admits to using injected drugs • On exam he has a stage 3 hemorrhoid (prolapses with minimal pressure) that has some ulceration and scarring on the mucosa ____________________ Learning point: Many IDUs sell anal sex for drugs. Advanced hemorrhoids are not uncommon among IDUs and are a result of repeated anal trauma Anal Fissures may develop from this trauma as well Anal Symptoms Courtesy CDC, USA Anal Warts Anal Fissure TREATMENT OF GONORRHOEA Uncomplicated Anal/ Genital Infection ANAL SYMPTOMS Discharge Confirm on exam Discharge Confirmed Yes Treat for Gonorrhoea and Chlamydia No Ulcers or blisters seen Pain Cefixime 400 mg orally once only Ceftriaxone 125 mg IM once only No Examination (use proctoscope if cause not seen on inspection) only OR OR No abnormality Anal symptoms Ciprofloxacin 500 mg orally once Warts OR Supportive/ symptomatic care Spectinomycin 2 gm IM once only Disseminated Gonococcal infection Ceftriaxone 1 gm IM or intravenous once daily for 7 days OR Spectinomycin 2 gm IM twice Yes Treat for HSV-2 Test and treat for Syphilis Wart removal/ needs observation for cancer daily for 7 days TREATMENT OF CHLAMYDIA Uncomplicated Anal/ Genital Infection Doxycycline 100 mg orally twice daily for 7 days OR Azithromycin 1 gm orally once only Alternative Regimens Amoxycillin 500 mg orally 3 times a day for 7 days OR Erythromycin 500 mg 4 times a day for 7 days OR Ofloxacin 400 mg orally twice a day for 7 days OR Tetracycline 500 mg orally 4 times a day for 7 days TREATMENT OF HSV-2 Treatment of First Episode: Acyclovir 400 mg 3 times a day for 7 days Treatment of Recurrent Episodes: Acyclovir 400 mg 3 times a day for 5 days Suppressive therapy: Acyclovir 400 mg twice a day continuously 4 Cs: 1.Compliance Counseling 2.Promote & provide Condoms 3.Counseling for STI prevention, HIV testing; Educate and Reassure patient 4.Partner (Contact) treatment Hemorrhoids (piles) seen Treat for Hemorrhoids (piles) Rectal Fissures Refer for Surgical evaluation TREATMENT FOR WARTS Treatment is meant for external genitalia and vaginal. Please refer to gynaecologic specialist for cervical warts Provider administered: Podophyllin 10-25% in compound of tincture or benzoin. Apply carefully avoiding normal tissue. External genital genitalia should be washed thoroughly in 1-4 hours. Allow the applied medicine to dry before removing speculum. Repeat application weekly as needed. OR Cryotherapy (when available). Repeat after 1-2 weeks as needed Vaginal Discharge • Vaginal Discharge is a common complaint among women • Critical point: Do not treat women that don’t present with this complaint (ie Vaginal discharge is not the reason why they came to see you) • Critical point: Assessment of risk • High risk > Treat for cervicitis otherwise for vaginitis • Speculum exam does not improve Dx • HSV-2 can also cause rare discharge. Treatment nonresponders must be re-assessed for risk and for HSV-2 Tx • Asking about amount of discharge or smell may help distinguish cervicits from vaginits Vaginal Discharge: Causes Vaginitis Cervicitis Caused by Trichomoniasis (TV), Candidiasis and Bacterial Vaginosis Caused by Gonorrhoea and Chlamydia Most common cause of vaginal discharge Less common cause of vaginal discharge Easy to diagnose Difficult to diagnose No complications Major complications Treatment of partner unnecessary, except for TV Need to treat partner Clinical Case • 21 y/o married mother of 2 children presents with a sore throat • On a comprehensive review of systems she admits to having a vaginal discharge • On exam there is a scant vaginal discharge • Clinical point: This is likely physiological discharge and should not be treated Clinical Case • A 22 y/o mother of 1 child presents with vaginal discharge • She describes some scant odor to the discharge which also itches • On rapport building she admits that she occasionally has sex with a neighbor for money to make ends meet • Clinical point: This is likely Cervicitis. Note that the critical point is the assessment of risk Clinical Case • 34 y/o somewhat obese woman presents with vaginal itching and discomfort • One further questioning she also admits noticing a vaginal discharge • On rapport building there is no history of risky sex behavior • Clinical point: this is likely Candidiasis, this woman may have diabetes although having diabetes is not necessary for candidiasis Treat for Gonorrhoea and Chlamydia VAGINAL DISCHARGE Patient complains of vaginal discharge, vulval itching or burning No Yes History, examination and Risk assessment* High NG/CT prevalence in community or high individual risk profile Lower abdominal pain Yes TREATMENT OF GONORRHOEA Uncomplicated Anal/ Genital Infection Ciprofloxacin 500 mg orally once only OR Cefixime 400 mg orally once only OR Ceftriaxone 125 mg IM once only No OR Spectinomycin 2 gm IM once only Yes Treat for BV/ Trichomonas Use Lower Abdominal pain flowchart Abnormal discharge or vulval erythema Disseminated Gonococcal infection Ceftriaxone 1 gm IM or intravenous once daily for 7 days OR Spectinomycin 2 gm IM twice daily for 7 days No Use Appropriate flowchart *Risk factors assessed should include: Personal sexual history (including extramarital sex) High risk group membership Community factors such as STI prevalence in community. Vulval edema/curd-like discharge, erythema, excoriations present No No Yes Reassure patient Provide analgesics if needed 4 Cs Treat for Candida 4 Cs: 1.Compliance Counseling 2.Promote & provide Condoms 3.Counseling for STI prevention, HIV testing; Educate and Reassure patient 4.Partner (Contact) treatment Uncomplicated Anal/ Genital Infection Doxycycline 100 mg orally twice daily for 7 days OR Azithromycin 1 gm orally once only Alternative Regimens Amoxycillin 500 mg orally 3 times a day for 7 days OR Erythromycin 500 mg 4 times a day for 7 days OR Ofloxacin 400 mg orally twice a day for 7 days OR Tetracycline 500 mg orally 4 times a day for 7 days TREATMENT OF BACTERIAL VAGINOSIS Metronidazole 2 gm orally once (also treats Trichomonas) OR Yes Any other genital disease TREATMENT OF CHLAMYDIA TREATMENT OF CANDIDA Miconazole or clotrimazole 200 mg intarvaginally daily for 3 days OR Clotrimazole 500 mg intravaginallly once OR Fluconazole 150 mg orally once Alternate Regimen Nystatin 100,000 IU intarvaginally daily for 14 days Clindamycin 2% vaginal cream, 5 gm intravaginally at bedtime for 7 days OR Metronidazole 0.75% gel, 5 gm intravaginally twice daily for 7 days OR Clindamycin 300 mg orally twice daily for 7 days Treatment during Pregnancy First Trimester (only if treatment is imperative): Metronidazole 2 gm orally once 2nd or 3rd trimesters: Metronidazole 200- 250 mg 3 times a day for 7 days Alternative regimen Metronidazole 2 gm orally once OR Clindamycin 300 mg orally twice daily for 7 days OR Metronidazole 0.75% gel, 5 gm intravaginally twice daily for 7 days Lower Abdominal Pain • Main concerns: – PID (infectious) – Retained placenta/ dead fetus/ other products of conception • Critical finding: Cervical Motion Tenderness • Prompt referral for non-responders is critical • Hospitalization important for serious patients Clinical Case • 32 y/o woman presents with lower abdominal pain for past 4 days • She denies any history of risky sex (was asked properly, with respect and tact) • She did have increase in vaginal discharge 3 weeks ago (she usually notices some discharge every month) but was busy helping her husband with some essential house work before he started another truck trip to Afghanistan • On exam there is cervical motion tenderness • Clinical point: This is likely PID Clinical Case • A 28 y/o woman presents with lower abdominal pain for 6 months - on and off • Her abdominal pain is not related to meals and she does not have diarrhea (if anything she often does not need to go to bathroom for 2-3 days) • There is no risky sex behavior • She lives in a household of 14 people and her husband is the only bread earner • There is no cervical motion tenderness • Clinical point: This is unlikely to be infectious Lower Abdominal Pain Criteria for hospitalization: • Pregnant patient • Cannot exclude surgical emergencies (ie appendicitis) • Severe illness: Nausea and vomiting or Fever >39oC, • Severe pain (enough to interfere with daily life) • No response to oral medicines • Unable to take or can not tolerate oral medicines • Evidence of a tubo-ovarian abscess OUTPATIENT TREATMENT OF LOWER ABDOMINAL PAIN LOWER ABDOMINAL PAIN Ceftriaxone 125 mg IM once only OR Appropriate surgical or gynecological referral Patient complains of lower abdominal pain History and examination (including gynecological exam) Any of the following present: Missed or overdue period Recent delivery/ abortion/ miscarriage Adnominal guarding and/or rebound tenderness Abnormal vaginal bleeding Abdominal mass intrauterine device Spectinomycin 2 gm IM once only PLUS Doxycycline 100 mg orally twice daily for 7 days Yes No Cervical motion tenderness or lower abdominal tenderness and vaginal discharge No Yes OR Any other illness found Appropriate management Refer or Specialist care • Manage for PID • 4 Cs • Review in 5 days No Patient improved Yes 4 Cs: 1.Compliance Counseling 2.Promote & provide Condoms 3.Counseling for STI prevention, HIV testing; Educate and Reassure patient 4.Partner (Contact) treatment Tetracycline 500 mg orally 4 times a day for 7 days (both Doxycylcine and Tetracycline are contraindicated for pregnant women) PLUS Metronidazole 400 mg orally twice daily for 14 days ALL PATIENTS NOT IMPROVING WITH OUTPATIENT THERAPY MUST BE ADMITTED FOR FURTHER TREATMENT Continue until treatment completed Reassure patient Provide analgesics if needed 4 Cs Ask patient to return as needed Common side effects of medicines used Acyclovir: Rare side effects in patients treated short-term with acyclovir are nausea, vomiting, and headache. Long-term treatment has the additional potential for rash and diarrhea. Azithromycin: Azithromycin is generally well tolerated. The most common side effects are diarrhea or loose stools, nausea, abdominal pain, and vomiting, each of which may occur in fewer than one in twenty persons who receive Azithromycin. Rarer side effects include abnormal liver tests, allergic reactions, and nervousness. Ceftriaxone: If administering Ceftriaxone into a muscle, it may be mixed with Lidocaine (Xylocaine, Lignocaine) to reduce pain at the injection site. Milder symptoms are: Diarrhea, stomach pain, upset stomach, vomiting. More severe symptoms include: unusual bleeding or bruising, difficulty breathing, itching, rash, hives, sore mouth or throat. Cefixime: Cefixime is generally well tolerated and side effects are usually transient. Reported side effects include diarrhea, pseudomembranous colitis (can occur even after cefixime is stopped) nausea, abdominal pain, vomiting, skin rash, fever, joint pain and arthritis, abnormal liver tests, vaginitis, itching, headaches, and dizziness. Clindamycin: Mild diarrhea or stomach upset may occur. If any of these effects persist or worsen, they should be observed carefully. Although unlikely, vaginal pain/itching/discharge may occur or worsen. These symptoms may be due to a new vaginal infection (e.g., yeast/fungal infection, trichomonas infection). This medication may infrequently cause a fungal infection in another part of the body (e.g., oral thrush). This may manifest as a change in vaginal discharge, white patches in your mouth, or other new symptoms. Many people using this medication do not have serious side effects. Serious side effects include: pain on urination, lower back pain, menstrual problems, abnormal vaginal bleeding. A very small amount of this medication may be absorbed into bloodstream and may rarely cause a severe intestinal condition (pseudomembranous colitis) due to a resistant bacterium. This condition may occur while receiving therapy or even weeks after treatment has stopped. Do not use anti-diarrhea products or narcotic pain medications if you suspect that the patient has this condition because these products may make them worse. Major signs of pseudomembranous colitis are persistent diarrhea, abdominal or stomach pain/cramping, or blood/mucus in stool. A very serious allergic reaction to this drug is unlikely, but requires immediate medical attention if it occurs. Symptoms of a serious allergic reaction may include: rash, itching, swelling, severe dizziness, trouble breathing. Fluconazole: Up to 25% develop side effects from this medication. Headaches, nausea, abdominal pain, diarrhea or dizziness are common. Severe skin rash may occur but is uncommon. Miconazole: Irritation and burning have been reported by patients using topical or vaginal miconazole Clotrimazole: The most commonly noted side effects associated with clotrimazole are local redness, stinging, blistering, peeling, swelling, itching, hives, or burning at the area of application. All of these are quite unusual, however. Tinidazole: Tinidazole may cause side effects. Consider stopping it if any of these symptoms are severe or do not go away: sharp, unpleasant metallic taste, upset stomach, vomiting, loss of appetite, constipation, stomach pain or cramps, headache, tiredness or weakness, dizziness. Some side effects can be serious. The following symptoms are uncommon, but require that the medicine must be stopped immediately: seizures, numbness or tingling of hands or feet, rash, hives, swelling of the face, throat, tongue, lips, eyes, hands, feet, ankles, or lower legs, hoarseness, difficulty swallowing or breathing Nystatin: diarrhea, nausea, gas, or vomiting as until the body adjusts to the medication. If these symptoms persist or get worse consider stopping the medicine. Doxycycline: Doxycycline is generally well-tolerated. The most common side effects are diarrhea or loose stools, nausea, abdominal pain, and vomiting. Tetracyclines, such as doxycycline, may cause tooth discoloration if used in persons below 8 years of age. Exaggerated sunburn can occur with tetracyclines; therefore, sunlight should be minimized during treatment. Tetracycline: Tetracycline is generally well-tolerated. The most common side effects are diarrhea or loose stools, nausea, abdominal pain, and vomiting. Tetracyclines may cause discoloration of teeth if used in patients below 8 years of age. Exaggerated sunburn can occur with tetracyclines; therefore, sunlight should be minimized during treatment Metronidazole: Metronidazole is generally well tolerated with appropriate use. Serious side effects of metronidazole are rare; and include seizures and damage of nerves resulting in numbness and tingling of extremities (peripheral neuropathy). Metronidazole should be stopped if these symptoms appear. Minor side effects include nausea, headaches, loss of appetite, a metallic taste, and rarely a rash. Ciprofloxacin: Nausea, vomiting, diarrhea, abdominal pain, rash, headache, and restlessness. Rare allergic reactions have been described, such as hives and anaphylaxis (shock) Levofloxacin: The most frequently reported side events are nausea or vomiting, diarrhea, headache, and constipation. Less common side effects include difficulty sleeping, dizziness, abdominal pain, rash, abdominal gas, and itching. Ofloxacin: The most frequent side effects include nausea, vomiting, diarrhea, insomnia, headache, dizziness, itching, and vaginitis in women. Rare allergic reactions have been described, such as hives and anaphylaxis (shock). Symptoms of nervous system stimulation, such as anxiety, euphoria, and hallucinations have rarely been reported. Penicillin: This medication may cause mild diarrhea, stomach upset, nausea, vomiting or irritation at injection site during the first few days. If this irritation worsens or persist for more than a few days, stop the medicine. Medicine should be stopped if patient develops: watery diarrhea, stomach cramps, fever, unusual bleeding or bruising, yellowing of the eyes or skin, unusual tiredness or weakness. In the unlikely event of an allergic reaction to this drug, appropriate care for anaphylaxis should be provided. Symptoms of an allergic reaction include: wheezing, difficulty breathing, skin rash, hives, itching. Podophyllin Swelling, pain, burning, itching, peeling skin, small sores, or headache may occur. Most serious side effect is bleeding.