joints and synovial movements
advertisement

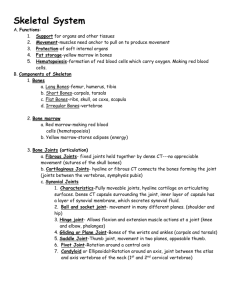
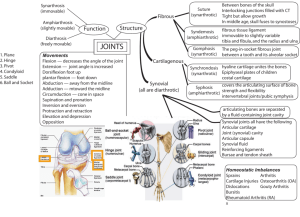
Objectives for Chapter 8 1. List the definition and functions of joints. 2. Describe the types of joints based on structural classification. 3. Describe the types of joints based on functional classification. 4. Define all types of fibrous and cartilaginous joints and know which group they are in. 5. Describe the 5 features of a synovial joint and be able to label a picture of a synovial joint. 6. Define bursae and tendon sheaths. 7. Describe the 3 factors that stabilize synovial joints and know which is the most important. 8. Define the following joint movements: gliding, flexion, extension, abduction, adduction, circumduction, rotation. 9. Describe the following joint injuries: sprain, cartilage injuries, dislocation, bursitis, and tendonitis. Joints Joints (Articulations): Sites where two or more bones meet. Two functions: 1. Secure bones together and 2. Allow rigid skeleton to move. With the exception of the hyoid bone, every bone forms a joint with at least one other bone. Joint Classification: Structural classification: Based on the material binding the bones together Presence or absence of a joint cavity Examples: fibrous, cartilaginous, synovial joints Functional classification: Based on the amount of movement allowed synarthroses - immovable joints amphiarthroses - slightly movable joints diarthroses - freely movable joints Freely movable joints predominate in the limbs. Immovable and slightly movable joints are found in the axial skeleton. Fibrous joints are immovable. Synovial joints are freely movable. Cartilaginous joints have both rigid and slightly movable examples. Fibrous joints: Bones are joined by fibrous tissue. No joint cavity present. Most are synarthrotic (no movement). Three types based on type and length of intervening fibers (sutures, syndesmoses, gomphoses). Sutures: Articulating bone edges either overlap or interlock. Junctions completely filled by very short connective tissue fibers. Rigid. Examples are found between bones of the cranium. Syndesmoses: Bones are connected by a cord or sheet of fibrous tissue (ligament or interosseous membrane). Amount of movement increases with the length of the connecting fibers (note: compare the radius-ulna interosseous membrane with that of the tibia-fibula). Gomphoses: Refers to the way teeth are embedded in their sockets. Connection is by a short periodontal ligament Cartilaginous joints: Articulating bones are united by cartilage. Lack a joint cavity. Two types (synchondroses and symphyses). Synchondroses: Bones are united by a bar or plate of hyaline cartilage. During youth, provides sites and means for bone growth, while contributing to skeletal flexibility. After bone growth ends, ossification occurs and they become immovable. Most common example - epiphyseal plates of long bones, joint between 1st rib and manubrium Symphyses: Articular surfaces of the bones are covered with articular hyaline cartilage which is fused to a pad or plate of fibrocartilage. Fibrocartilage acts as a shock absorber and permits limited movement. Designed for strength with flexibility. Examples: intervertebral discs, pubic symphysis. Synovial Joints: Articulating bones are separated by a fluid-filled joint cavity. Permits freedom of movement - diarthrotic joints. Examples: all joints of the limbs, most joints of the body. Five distinguishing features: 1. Articular cartilage - covers opposing bone surfaces. 2. Joint cavity. 3. Articular capsule - cavity enclosed by a double-layered articular capsule. Synovial membrane lines the capsule internally and covers all internal joint surfaces that are not hyaline cartilage. 4. Synovial fluid: provides a slippery weight-bearing film that reduces friction. Also provides nourishment to the cartilage. 5. Reinforcing ligaments: joints reinforced and strengthened by a number of ligaments. Certain synovial joints such as the hip and knee have cushioning fatty pads between the fibrous capsule and the synovial membrane or bone. Others have discs or wedges of fibrocartilage separating the articular surfaces of the bones. The articular discs improve the fit between the articulating bone ends, making the joint more stable. Found in the knee, jaw, and sternoclavicular joints. Bursae and Tendon Sheaths: Not part of synovial joints but frequently found associated with them. Act as "ball bearings" to prevent friction on adjacent structures. Bursae are flattened fibrous sacs lined with synovial membrane and containing a thin film of synovial fluid. Bursae are common in sites where ligaments, muscles, skin, or muscle tendons overlie and rub against bone. Tendon sheaths are elongated bursae that wrap completely around a tendon subjected to friction. Joints must be stabilized so that they do not dislocate. The stability of a synovial joint depends on three factors: 1. nature of articular surface - shapes of articular surfaces determine what movements are possible. 2. number and positioning of ligaments - Ligaments unite the bones, help direct bone movement, and prevent excessive or undesirable motion. 3. muscle tone - Muscle tendons that cross the joint are the most important stabilizing factor. The tendons are kept taut at all times by the tone of their muscles. Muscle tone is extremely important in reinforcing the shoulder and knee joints. Movements Allowed by Synovial Joints: Movements can be described in directional terms relative to the lines, or axes, around which the body part moves and the planes of space along which the movement occurs. Range of motion allowed by synovial joints varies from: 1. nonaxial- slipping motion only 2. uniaxial - movement in one plane 3. multiaxial - movement in or around all three planes of space or axes Three general types of movements: 1. gliding - intercarpal/tarsal, intervertebral, sternoclavicular joints. 2. angular - change the angle between two bones. flexion (reduce angle), extension (increase angle), abduction (move laterally), adduction (move medially), circumduction (movement of the distal portion of a limb in a circular pattern so that the movement of the entire limb describes a cone.) 3. rotation - turning movement of a bone around its own long axis. Only movement allowed by atlas-axis joint; common at the hip and shoulder joints. Common Joint Injuries: 1. Sprain - ligaments reinforcing a joint are stretched or torn. Most common sites are the lumbar region of the spine, ankle, and the knee. Partially torn ligaments will repair themselves. Heal slowly and tend to be painful and immobilizing. Completely ruptured ligaments must be repaired surgically and quickly, because the inflammatory response in the joint will turn the injured ligament to mush. 2. Cartilage injuries involve tearing of the knee menisci due to high pressure and twisting motions occurring simultaneously. Being avascular tissue, cartilage rarely can repair itself. Fragments can interfere with joint function by causing locking or binding of the joint. Must be removed surgically (usually arthroscopically). Removal of some or all of a meniscus does not severely impair knee joint mobility, but the joint is definitely less stable. 3. Dislocation - occurs when bones are forced out of their normal positions at a joint. Usually accompanied by sprains, inflammation, and joint immobilization.Common contact sports injury. Joints of the shoulders, fingers, and thumbs are commonly dislocated. Must be reduced (returned to their proper position). 4. Bursitis and Tendonitis - inflammation of a bursa caused by excessive stress or friction. Caused by: falling on one's knee (housemaid's knee or water on the knee), prolonged leaning on one's elbows (student's elbow or olecranon bursitis), bacterial infection. Symptoms include pain made worse by movement, redness, swelling. Tendonitis is inflammation of tendon sheaths. Its causes, symptoms, and treatment are the similar to that for bursitis