Surgical Approaches for Rib Fracture Fixation
advertisement

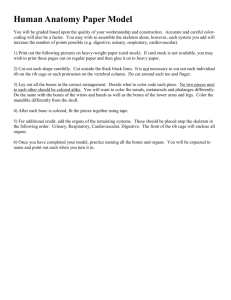
TECHNICAL TRICK Surgical Approaches for Rib Fracture Fixation Benjamin C. Taylor, MD,* Bruce G. French, MD,* and T. Ty Fowler, MD† Summary: Operative management of thoracic injuries is an increasingly accepted technique, with multiple reports of improved patient outcomes as compared with nonoperative treatment. Despite the evolving support of rib fracture fixation, descriptions of surgical approaches and tactics remain limited. We present this information to allow surgeons to begin or improve treatment of these injuries. In addition, we present the initial treatment results of a series of 21 patients treated with the approaches described within. Key Words: rib fracture, flail chest, surgical approach, rib fixation (J Orthop Trauma 2013;27:e168–e173) INTRODUCTION Among trauma patients, thoracic injury ranks behind only head trauma as a cause of injury-related death in the United States.1 Rib fractures carry significant clinical importance, as mortality is directly correlated to the number of rib fractures present,2 and the simple presence of flail chest alone has a reported mortality rate of up to 33%.3 Conservative treatment generally consists of ventilator-assisted respiratory support, tracheostomy, pulmonary toilet, narcotic pain control, and epidural anesthesia4 but is associated with significant risks of pneumonia, septicemia, prolonged hospitalization, pulmonary barotrauma, and chronic pain and long-term pulmonary dysfunction.5–9 Evidence continues to mount regarding improved shortand medium-term outcomes after operative treatment of rib fixation. Decreased ventilator times, intensive care unit stay length, and length of hospitalization have all been reported in several prospective and retrospective case series, with improvements in pulmonary function, chest wall geometry, pneumonia incidence, and need for tracheostomy noted with operative stabilization of flail chest.10–16 Despite the positive results noted in the multiple series from different centers, operative fixation of rib fractures and flail chest injuries remains an underutilized procedure.17,18 This underutilization seems to be a result of most surgeons being unfamiliar with either the literature surrounding Accepted for publication December 19, 2012. From the *Department of Orthopedic Surgery, Grant Medical Center, Columbus, OH; †Department of Orthopaedic Surgery, Mount Carmel Medical Center, Columbus, OH. B.G. French is a consultant for Biomet and is on the speaker’s bureau for Synthes. B.C. Taylor is on the editorial board of orthobullets.com. The other author reports no conflict of interest. Supplemental digital content is available for this article. Direct URL citations appear in the printed text and are provided in the HTML and PDF versions this article on the journal’s Web site (www.jorthotrauma.com). Reprints: Benjamin C. Taylor, MD, 285 East State St, Suite 500, Columbus, OH 43215 (e-mail: drbentaylor@gmail.com). Copyright © 2013 by Lippincott Williams & Wilkins e168 | www.jorthotrauma.com flail chest fixation, chest wall anatomy, and surgical approaches or fixation techniques/instrumentation.17,18 This article attempts to better delineate the surgical approaches available to the operating surgeon, to provide a means to minimize a surgeon’s possible unfamiliarity with thoracic approaches. This will hopefully lead to improved patient outcomes through surgical treatment of flail chest when indicated. APPROACHES OVERVIEW As with any surgical approach, an understanding of the regional anatomy is required for minimizing iatrogenic injury. Surface topography is used to facilitate surgical incision planning, with several reliable landmarks noted. The superior angle of the scapula typically resides at T3, whereas the inferior angle of the scapula is usually seen over the seventh rib. Anteriorly, the inferior aspect of the pectoralis major corresponds to the fifth rib, whereas the superior-most aspect of the serratus anterior indicates the sixth rib. Surgical planning involves evaluation of plain radiographs and traditional computed tomography (CT), but it seems that 3-dimensional CT has some benefit in detecting rib fractures.19 With 3-dimensional CT, the surgeon is able to completely evaluate the bony thorax and can plan a more focused, or direct, approach to the segments requiring fixation, potentially obviating the need for a full thoracotomy approach. STANDARD POSTEROLATERAL THORACOTOMY The standard posterolateral thoracotomy is an approach familiar to most cardiothoracic and general surgeons but is not typically used by the orthopedic surgeon. This approach allows access to posterior, posterolateral, and lateral rib fractures, with access anteriorly with extension of the transverse or oblique limb of the incision. In this approach, the patient is placed in the lateral decubitus position, with the arm placed on an overhead armboard for stability. If desired, the ipsilateral arm may be prepped to allow intraoperative manipulation; forward flexion of the shoulder on the overhead armboard can lead to scapular protraction or lateralization, which can limit intraoperative fracture visualization and manipulation. In addition, if the surgical table can be broken, or extended, at the thoracic level, this may serve to further improve visualization by allowing the hemithorax to “open up” with the contralateral deviation. The skin incision is begun at an equidistant point between the spinous processes and the medial border of the scapula and is continued caudally (Fig. 1A). The inferior extent of this incision depends on the need for exposure of the lower ribs; typically, this aspect of the incision is stopped at 1.5–2 cm caudal to the inferior angle of the scapula. The incision is then J Orthop Trauma ! Volume 27, Number 7, July 2013 J Orthop Trauma ! Volume 27, Number 7, July 2013 Surgical Approaches for Rib Fracture Fixation FIGURE 1. A, Patient in the lateral decubitus position with anatomic landmarks and incision line drawn out. The patient’s head is to the right. B, Scapular retractor being used after incision of the latissimus dorsi muscle (white arrow). The rhomboid major muscle is intact at the right edge of the retractor. C, Blunt splitting of the serratus anterior muscle for fracture access is easily done (black arrow). The overlying latissimus dorsi muscle has been transected here for access (white arrow). D, The addition of percutaneous “stab” incisions are frequently needed for placement of more caudal or anterior fixation. carried laterally in a curvilinear fashion, with the direction of angulation and length of incision decided by the need for surgical access. This curvilinear extension generally mirrors the course of the lower ribs and can be extended anteriorly to the sternum if needed. Superficial dissection reveals the trapezius muscle in the vertical limb of the incision, and this muscle can generally be retracted medially and cranially without difficulty. Deep to this and medial to the scapula is the rhomboid major, which is also typically easily elevated off the posterior thorax. Care must be taken to limit the surgical morbidity to this muscle, as lateral scapular winging will ensue with significant devitalization or transection. The fibers of the latissimus dorsi are then identified superficially and caudally as they extend obliquely from their origin on the thoracic spinous processes and thoracolumbar fascia toward the humerus. The latissimus is lifted from the underlying muscles and transected as needed for surgical access; the enveloping fascia is protected for later repair (Fig. 1B). The serratus anterior is then seen and the muscle is split in line with its fibers along the thorax to gain access to displaced posterolateral rib fractures (Fig. 1C). Care must be taken with muscle splitting in the midaxillary line, as the long thoracic nerve is seen superficial to the muscle and can be injured with errant dissection. A Davidson scapular retractor is then used deep to the scapula and subscapularis muscle, and visualization can also be aided by manipulation of the ipsilateral arm, as changes in shoulder position will lead to changes in scapulothoracic positioning. Further anterior and caudal dissection will lead to the external oblique muscle, which is made of fibers that parallel the lateral and anterolateral ribs, but run at nearly right angles to the anterior ribs. This muscle is typically split in line with it’s fibers, but full anterior exposure of a single rib may require several small muscle splits because of the mismatch of the ! 2013 Lippincott Williams & Wilkins course of the rib and that of the muscle fibers. The anterior rib fractures may also be accessed via additional smaller or percutaneous incisions to minimize morbidity (Fig. 1D). Access to the posterior most ribs and the costovertebral junction requires either transection of some of the posterior trapezius muscle fibers or elevation of its origin off of the thoracic spinous processes. Similarly, the rhomboid major muscle requires splitting or transection for access to the posterior aspects of ribs 2–5. The midline paraspinal musculature, which roughly parallels the spine, should be simply elevated off the injured area and not transected in efforts to minimize subsequent back pain and weakness. MUSCLE SPARING THORACOTOMY Although muscle-sparing thoracotomy for lung resection has been shown in several studies to have no advantage as compared with the traditional muscle-cutting approach,20–23 the differences remain undetermined when used for rib fracture fixation. It is possible and even likely that the rib spreading needed for access in these cases introduces a confounding variable that prevents direct comparison to rib fixation cases. Pure muscle transection for surgical access to rib fractures is not without complication; alterations in shoulder function and cosmesis can be seen (Fig. 2). The muscle sparing thoracotomy approach uses the same positioning and incision as described in the previous section, but differs in the deep dissection (Fig. 3A). The incision is taken down to the trapezius and latissimus muscle fascia, and the fascia is elevated off the deeper muscle layers to allow visualization of the muscular intervals (see Video, Supplemental Digital Content 1, http://links.lww.com/BOT/A83 which demonstrates this surgical approach). The subcutaneous www.jorthotrauma.com | e169 Taylor et al J Orthop Trauma ! Volume 27, Number 7, July 2013 FIGURE 2. This clinical photograph shows significant left-sided asymmetry and muscle wasting after long-term follow-up of a muscle-transecting thoracic procedure. elevation should be minimized, however, to minimize risk of postoperative seroma formation.20,21 The triangle of auscultation, which is bordered superiomedially by the trapezius, inferiorly by the latissimus dorsi, and laterally by the scapula, is immediately identified and allows for direct access to the posterior rib cage (Fig. 3B). The surrounding muscles are retracted with relative ease, allowing direct access to the posterior aspects of ribs 4–8 (Fig. 3C). The subscapular bursa can be bluntly entered if needed, and retractors placed under the subscapularis and serratus anterior muscles to allow visualization of the subscapular thorax. Access to more anterior fractures is done with a blunt split of the latissimus dorsi fibers (Fig. 3D); lateral and anterolateral fractures may also require posterior retraction of the latissimus dorsi, as well as blunt splitting of the underlying serratus anterior muscle (Fig. 3E). More cephalad posterior and posterolateral fractures will require blunt splitting of the trapezius and underlying rhomboid major muscle in line with their respective fibers to allow access. However, even in muscular individuals, generally, no splitting of the trapezius or rhomboid muscles is needed unless surgical fixation of the fourth rib or above is performed. The posterior aspect of the ribs near their costovertebral articulation may be approached with elevation and midline retraction of the paraspinal musculature. No deep muscular interval closure is needed for this approach, but suturing the deep aspect of the full thickness skin flaps down to the appropriate muscle will limit postoperative “dead space” and limit postoperative hematoma or seroma formation. Alternatively, the full thickness flap may be closed over a drain. AXILLARY APPROACH This approach is used for anterolateral rib fractures requiring fixation. It affords a fairly large exposure of the anterolateral thorax and direct visualization of the long thoracic e170 | www.jorthotrauma.com nerve. Unfortunately, it does not allow access to the chondral aspect of the ribs anteriorly without significant anterior extension of the incision, although also limiting the surgical visualization of posterolateral rib fractures, and therefore is typically used only in situations that require a broad exposure for reduction and fixation of multiple anterolateral rib fractures. The patient is placed either in a true lateral decubitus position or alternatively in a “sloppy” lateral position, with the injured side elevated approximately 45 degrees. A vertical incision is made approximately 1.5 cm lateral to the lateral border of the scapula, and this is carried inferiorly down to a level approximately 1–2 ribs above the level of required fixation. The incision is then carried anteriorly in a transverse fashion as needed for appropriate exposure (Fig. 4A). The long thoracic nerve is identified on the lateral aspect of the serratus anterior and protected throughout the procedure to minimize postoperative scapular winging (Fig. 4B). The latissimus dorsi can be seen posteriorly, and a retractor can be placed under the muscle here to improve visualization, if necessary. The displaced rib fractures in this region typically injure the serratus anterior, but this muscle can be easily split in line with its fibers to gain access to the rib fractures for reduction and fixation. Extension anteriorly requires blunt splitting of the external oblique muscle or extension into a pectoralis-lifting approach, which will be described below. INFRAMAMMARY/PECTORALIS-LIFTING APPROACH With this approach, the patient is placed in the supine position or if access is needed anterolaterally, a small bump can be placed under the ipsilateral hemithorax to increase lateral access. The skin incision is made in the inframamillary crease for improved cosmesis (Fig. 5A) and access to the anterior ribs and costal cartilage can be obtained with lifting the breast tissue and pectoralis major muscle anteriorly and superiorly (Fig. 5B). The pectoralis minor muscle can be seen at its origin near the costochondral junctions of the third to fifth ribs and may require elevation for rib fixation. For more caudal access, the external oblique muscle is seen caudal to the pectoralis major, and this muscle can be safely split in line with its fibers for access to several additional caudal ribs without enlarging or adding a separate incision. If dissection is needed laterally, the serratus anterior will be encountered and can be split in line with its fibers to gain access to the ribs if needed. This approach can be extended posterolaterally into either the axillary or standard thoracotomy approach. RESULTS Twenty-one patients with flail chest between June 2010 and June 2011 were managed with the operative approaches and internal fixation outlined in this manuscript. The patient population averaged 51.5 (range, 18–90) years and was predominately male (66.7%). Motor vehicle collisions (13) and falls (7) were the prime mechanisms of injury. These patients fractured a mean of 6.0 (range, 3–10) ribs, with a mean of 3.4 (range, 0–7) consecutive segmental fractures. In addition, 33.3% of the patients sustained a mean of 3.9 (range, 0–8) contralateral rib ! 2013 Lippincott Williams & Wilkins J Orthop Trauma ! Volume 27, Number 7, July 2013 Surgical Approaches for Rib Fracture Fixation FIGURE 3. A, The patient in the lateral decubitus position with the scapular borders drawn out, the spinous processes marked with dots, and the proposed incision line drawn as well. The patient’s head is to the left. B, The superficial dissection reveals the triangle of auscultation (white arrowhead), bordered by the latissimus dorsi (black arrow), trapezius (white arrow), and scapula (black arrowhead). C, The latissimus dorsi (black arrow) is easily lifted off the thorax for access to the underlying thorax. D, The latissimus dorsi can also be split in line with its fibers for creation of different surgical windows, as shown here. E, The serratus anterior muscle (white arrows) can also be bluntly split in line with its fibers for anterior access. The latissimus dorsi (black arrows) is shown posterior to the serratus anterior; the patient’s head is to the right. fractures. These fractures were treated at a mean of 4.6 (range, 2–11) days after admission. The initial procedures were performed in conjunction with the general trauma surgeons, but as surgeon comfort with the technique improved, the general surgeon involvement dwindled to chest tube placement and management only. Six pectoralis-lifting approaches, 2 axillary approaches, 8 standard thoracotomy approaches, and 5 muscle-sparing thoracotomy approaches were used as described above. Estimated blood loss was an average of 98.1 (range, 25–400) mL, and operative time averaged 160.2 (range, 92–236) minutes. A mean of 4.7 (range, 2–7) ribs were plated per patient, requiring a mean of 5.7 (range, 2–12) plates. All fractures were stabilized with the MatrixRIB plating system (Synthes, West Chester, PA). All FIGURE 4. A, Superficial dissection of the axillary approach shows the latissimus dorsi (black arrow) in the posterior aspect of the approach, with the long thoracic nerve and lateral thoracic artery (white arrow) overlying the serratus anterior muscle. B, The serratus anterior muscle may be split in line with its fibers to allow access to the underlying rib fractures. The overlying long thoracic nerve should be identified and protected to minimize risk of iatrogenic denervation. ! 2013 Lippincott Williams & Wilkins www.jorthotrauma.com | e171 Taylor et al J Orthop Trauma ! Volume 27, Number 7, July 2013 FIGURE 5. A, The incision for the pectoralis-lifting approach should be located in the inframammary crease to improve scar cosmesis and minimize risk of injury to breast tissue. B, The pectoralis musculature (white arrow) is elevated off the thorax and retracted in a cephalad direction to allow for access to the more cephalad rib fractures. patients had placement of a chest tube to the ipsilateral thorax intraoperatively; an indwelling On-Q pain catheter (I-Flow, Lake Forest, CA) was also placed in a submuscular fashion to provide perioperative pain control. The On-Q pump was removed at 72 hours postoperatively, although the chest tube was followed by the general surgeons and removed when outputs were minimal on gravity suction. Immediate shoulder and thoracic range of motion was encouraged and facilitated postoperatively by physical therapists. Two patients (9.5%) required a tracheostomy for prolonged ventilator dependence, but no other perioperative complications were noted in this series. This patient cohort required a mean of 14.6 (range, 4–47) days in the hospital, postoperatively, with a mean intensive care unit stay of 5.2 (range, 0–13) days. Ventilator dependence was a mean of 4.8 (range, 0–26) days, with chest tube removal at a mean of 7.4 (range 0–28) days. Two patients were lost to follow-up before 12 months. All of the fractures went onto clinical and radiographic union at a mean of 3.4 (range 2–5) months. No soft tissue healing complications or infections were noted, and no complaints of intercostal neuralgia were seen. DISCUSSION Rib fracture fixation is increasingly used for treatment of flail chest, with increasing amounts of evidence published pointing to its efficacy in improving patient outcomes.3,4,10–17 Despite the emerging data, the descriptions of surgical approaches are largely poorly characterized in the published studies, and little attention is paid to the methods of exposure during these surgical cases. It is possible, and even likely, that the exposure plays a significant role in the rib fracture patient’s recovery and eventual outcome, but this currently remains unknown. No published evidence exists as to the functional outcomes of patients after differing approaches for rib fracture fixation, but there has been comparison of traditional and muscle-sparing techniques for thoracic and spinal surgeries. For posterolateral thoracotomies performed for lung resections and lobectomies, several randomized prospective studies have found that postoperative pain rates were similar, as were pulmonary function levels.20–23 The muscle-sparing technique was reported to have improved initial muscle strength in several of these studies, but no differences were seen between the patient groups in any of the studies by 1 month, postoperatively. The lack of difference between these 2 groups may be indirect evidence that other factors play a larger role in this patient population, as the ribs are forcibly spread apart and e172 | www.jorthotrauma.com intercostal nerves may be damaged in the process. In addition, emerging evidence exists showing that new techniques in closing the intercostal space (avoiding intercostal nerve compression) are able to significantly decrease postthoracotomy pain as compared with traditional techniques.24 In the spinal surgery literature, note is also made of the considerable complication rate after posterolateral thoracotomy. Lubelski et al25 reviewed the spinal literature regarding approaches to the thoracic spine, and noted a cumulative complication rate of 39% for the traditional thoracotomy approach, which was significantly higher than any of the other approaches to the thoracic spine. However, when further examined, muscle-sparing thoracotomy for access to the thoracic spine seems to have improved functional outcomes at final follow-up but requires more operative time.25–27 It remains unseen if patients undergoing rib fracture fixation would benefit from muscle-sparing techniques, and it is hoped that worthwhile data on this will be collected, analyzed, and published in the near future. In our series, we were able to safely provide improved pulmonary function, pain relief, and minimal complications via chest wall fixation using the approaches outlined here. We believe that rib fracture fixation is an emerging concept and one that will benefit patients greatly when carried out appropriately. Our descriptions of surgical approaches will hopefully allow further development of the techniques and even approaches themselves, leading to optimal patient outcomes. REFERENCES 1. Trunkey DD. Trauma. Accidental and intentional injuries account for more years of life lost in the U.S. than cancer and heart disease. Among the prescribed remedies are improved preventive efforts, speedier surgery and further research. Sci Am. 1983;249:28–35. 2. Flagel BT, Luchette FA, Reed L, et al. Half-a-dozen ribs: the breakpoint for mortality. Surgery. 2005;138:717–723. 3. Nirula R, Diaz JJ Jr, Trunkey DD, et al. Rib fracture repair: indications, technical issues, and future directions. World J Surg. 2009;33:14–22. 4. Fitzpatrick DC, Denard PJ, Phelan D, et al. Operative stabilization of flail chest injuries: review of literature and fixation options. Eur J Trauma Emerg Surg. 2010;36:427–433. 5. Ali BA, Sanfilippo F. Management of flail chest in trauma: analysis of risk factors affecting outcomes. ANZ J Surg. 2007;77:A93. 6. Sirmali M, Turut H, Topcu S, et al. A comprehensive analysis of traumatic rib fractures: morbidity, mortality, and management. Eur J Cardiothorac Surg. 2003;24:133–138. 7. Wanek S, Mayberry JC. Blunt thoracic trauma: flail chest, pulmonary contusion, and blast injury. Crit Care Clin. 2004;20:71–81. 8. Landerscaper J, Cogbill TH, Lindesmith LA. Long-term disability after flail chest injury. J Trauma. 1984;24:410–414. 9. Beal SL, Oreskovich MR. Long-term disability associated with flail chest injury. Am J Surg. 1985;150:324–326. ! 2013 Lippincott Williams & Wilkins J Orthop Trauma ! Volume 27, Number 7, July 2013 10. Althausen PL, Shannon S, Watts C, et al. Early surgical stabilization of flail chest with locked plate fixation. J Orthop Trauma. 2011;25:641–647. 11. Paris F, Tarazona V, Blasco E, et al. Surgical stabilization of traumatic flail chest. Thorax. 1975;30:521–527. 12. Ahmed Z, Mohyuddin Z. Management of flail chest injury: internal fixation versus endotracheal intubation and ventilation. J Thorac Cardiovasc Surg. 1995;110:1676–1680. 13. Granetzny A, Abd El-Aal M, Emam E, et al. Surgical versus conservative treatment of flail chest. Evaluation of the pulmonary status. Interact Cardiovasc Thorac Surg. 2005;4:583–587. 14. Tanaka H, Yukiola T, Yamaguti Y, et al. Surgical stabilization or internal pneumatic stabilization? A prospective randomized study of management of severe flail chest patients. J Trauma. 2002;52:727–732. 15. Reber PU, Kniemeyer HW, Ris HB. Reconstruction plates for internal fixation of flail chest. Ann Thorac Surg. 1998;66:2158. 16. Hellberg K, de Vivie ER, Fuchs K, et al. Stabilization of flail chest by compression osteosynthesis—experimental and clinical results. Thorac Cardiovasc Surg. 1981;29:275–281. 17. Richardson JD, Franklin HA, Heffley S, et al. Operative fixation of chest wall fractures: an underused procedure? Am Surg. 2007;73:591–596. 18. Mayberry JC, Ham LB, Schipper PH, et al. Surveyed opinion of American trauma, orthopedics, and thoracic surgeons on rib and sternal fracture repair. J Trauma. 2009;66:875–879. 19. Ishibashi H, Ohta S, Hirose M, et al. Benefit of three-dimensional computed tomography for traumatic rib fracture: easy to detect and explain rib fractures. Eur J Cardiothorac Surg. 2008;34:449. ! 2013 Lippincott Williams & Wilkins Surgical Approaches for Rib Fracture Fixation 20. Athanassiadi K, Kakaris S, Theakos N, et al. Muscle-sparing versus posterolateral thoracotomy: a prospective study. Eur J Cardiothorac Surg. 2007;31:496–499 21. Hazelrigg SR, Landreneau RJ, Boley TM, et al. The effect of musclesparing versus standard posterolateral thoracotomy on pulmonary function, muscle strength, and postoperative pain. J Thorac Cardiovasc Surg. 1991;101:394–400. 22. Akcali Y, Demir H, Tezcan B. The effect of standard posterolateral versus muscle-sparing thoracotomy on multiple parameters. Ann Thorac Surg. 2003;76:1050–1054. 23. Nosotti M, Baisi A, Mendogni P, et al. Muscle sparing versus posterolateral thoracotomy for pulmonary lobectomy: randomized controlled trial. Int Cardiovasc Thorac Surg. 2010;11:415–419. 24. Bayram AS, Ozcan M, Kaya FN, et al. Rib approximation without intercostal nerve compression reduces post-thoracotomy pain: a prospective randomized study. Eur J Cardiothorac Surg. 2011;39:570–574. 25. Lubelski D, Abdullah KG, Steinmetz MP, et al. Lateral extracavitary, costotransverectomy, and transthoracic thoracotomy approaches to the thoracic spine: review of techniques and complications. J Spinal Disord Tech. 2011. 26. Grewal H, Betz RR, D’Andrea LP, et al. A prospective comparison of thoracoscopic vs open anterior instrumentation and spinal fusion for idiopathic thoracic scoliosis in children. J Pediatr Surg. 2005;40: 153–156. 27. Soucy P, Bass J, Evans M. The muscle-sparing thoracotomy in infants and children. J Pediatr Surg. 1991;26:1323–1325. www.jorthotrauma.com | e173