1 Possible Essay Questions

Possible Essay Questions: The following are possible essay questions that are likely to be asked on exam III – total points from essay will be 15.
You are to pick one to write your essay on. To be
1 fully prepared you should be able to write on a number of these topics as well as the clinical applications topics (5-10 points) from your study guides. The exam will also contain general questions that pertain to the Key Medical Terms, blood tests and the lecture notes. All the best to you in your preparation and please do not hesitate to contact me if you have any questions about the material.
Possible Fifteen Point Essay Questions
1. Discuss the steps in the conduction system of the heart. Explain the function of autorhythmic cells and why the SA node is the pacemaker of the heart. Explain how action potentials in autorhythmic (pacemaker) cells are produced and how the parasympathetic and sympathetic nervous system can affect heart rate. Explain how action potentials in myocardial cells are produced. Explain what an ECG is, draw and label a typical ECG, and explain what causes each of the waves.
2. Describe the characteristics and functions of erythrocytes including a description of how oxygen and carbon dioxide are transported. Be sure to include the details of the chloride shift and how RBCs release oxygen at the tissues with emphasis on PO
2
and the Bohr Effect. Describe the mechanism of clot formation in a damaged blood vessel.
Explain how aspirin and plavix work to prevent blood clot formation.
3. Using a diagram, provide an overview of the main factors that determine mean arterial pressure. Be sure to include arrows and do not abbreviate words in the graph. Explain how the kidneys regulate blood volume and be sure to include details about antidiuretic hormone (ADH, vasopressin), aldosterone, and the rennin-angiotensin-aldosterone system. Explain how ACE Inhibitors work. Describe what circulatory shock is and explain the four main types. Define Edema and describe the 5 primary causes of edema.
Discuss the steps in the conduction system of the heart. Explain the function of autorhythmic cells and why the SA node is the pacemaker of the heart. Explain how action potentials in autorhythmic (pacemaker) cells are produced and how the parasympathetic and sympathetic nervous system can affect heart rate. Explain how action potentials in
2 myocardial cells are produced. Explain what an ECG is, draw and label a typical ECG, and explain what causes each of the waves.
Conduction System of the Heart: Steps in the Process
• Steps in the process :
1. Action potentials (wave of depolarization) originate in the SA node and spread over the Rt and Lt atria, signaling them to contract
• Without any input (neural or hormonal), the rate of SA node depolarization determines the heart rate (about
70 bpm).
2. Action potentials travel to the AV node and the depolarization wave is briefly delayed
– this allows the atria to complete contraction before the ventricles begin.
3. Action potentials travel down the AV bundle and right and left bundle branches.
4. Action potentials travel throughout the ventricles via the Purkinje fibers and the ventricular myocardial cells depolarize followed by contraction.
• Contraction begins at the apex of the heart and proceeds upward.
• The fibrous skeleton of the heart helps to electrically isolate the atria and the ventricles . The AV bundle is the only electrical connection between the atria and ventricles .
Autorhythmic Cells and the SA Node
• All of the autorhythmic cells found in the above conduction system have the ability to rhythmically and spontaneously depolarize.
• The SA node cells have the fastest rate of depolarization and therefore set the pace for autorhythmic cells and the rest of the heart. Thus, the SA node is known as the pacemaker of the heart .
– The action of cardiac muscle tissue contracting on its own in the absence of neural stimulation is called automaticity .
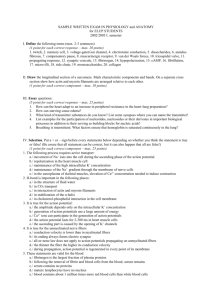
Production of Action Potentials in Autorhythmic Cells
• Action potentials of autorhythmic cells can be divided into three phases: Pacemaker
Potential Phase, Depolarization Phase, and Repolarization Phase
3
L-type Ca 2+ channels open
T-type Ca 2+ channels open,
I f channels close
Pacemaker potential phase: Pacemaker potentials are slow spontaneous depolarization's to threshold that triggers an action potential . They involve the movement of Na+, K+, and Ca 2+ ions.
o During diastole the cell starts out as being hyperpolarized (-60 mV) as a result of the preceding action potential. o This hyperpolarization opens special voltage-gated
Na+ channels which are also known as HCN channels and funny channels. These channels function to depolarize the cell by allowing a net movement of Na+ ions into the cell . At around -50 mV these channels close and T-type Ca 2+ channels open. o Transient Ca 2+ channels (T-type Ca 2+ channels) open at -50 mV further depolarizing the membrane to threshold (-40 mV) , at which time the T-type
Ca 2+ channels close.
Basis for the different names of these channels:
(A) Voltage gated Na+ channels: Channels are activated by a change in voltage
(hyperpolarization) but are permeable to both Na+ and K+ ions. However, the channel is more permeable to Na+ so it is the net movement of Na+ into the cell that causes the slow depolarization .
(B) HCN channels : H yperpolarizationactivated C yclic N ucleotide gated channels are so named because the channels have dual activation – are activated by both a change in voltage and by a cyclic nucleotide. Cyclic adenosine monophosphate (cAMP)
4 molecules bind directly to HCN channels and cause them to open. The importance of cAMP activation will be discussed in relation to sympathetic stimulation of heart rate.
(C) Funny (I f
) channels: The unusual behavior of these channels led to them being called funny, or I f
, channels. Typically, voltage-gated channels open when the membrane becomes less negative (depolarizes), but these unique channels open when the potential becomes more negative (hyperpolarizes) at the end of repolarization from the previous action potential. The dual activation and permeability to both Na+ and K+ ions also contribute to their “funny” properties.
• Depolarization Phase: At threshold (-40 mV), voltage-gated L-Type Ca 2+ channels open along the plasma membrane. o “L” stands for long-lasting o The inward diffusion of Ca 2+ produces the steep upward phase of the action potential.
• Repolarization Phase: Repolarization is produced by the closing of the voltage-gated Ltype Ca 2+ channels (at about -20 mV) and the opening of voltage-gated K+ channels allowing the outward diffusion of K+ and repolarizing the cell to a hyperpolarized state. o The hyperpolarized state triggers the opening of voltage gated Na+ channels and the process begins once again.
Effect of the parasympathetic and sympathetic nervous system on heart rate.
• Parasympathetic activation slows heart rate: ACh from parasympthetic axons (via the vagus nerve) bind to muscarinic receptors (G-protein coupled receptors) on SA nodal cells and cause the opening of K+ channels and the closing of T-type calcium channels .
– The opening of K+ channels slows the pacemaker depolarization because more positive K+ ions leave making the inside of the cell more negative.
– The closing of T-type Ca 2+ channels slows the pacemaker depolarization to threshold because less Ca 2+ moves into the cell
HCN Channel
5
• Sympathetic activation Increases Heart Rate:
Norepinephrine from sympathetic axons (via cardiac nerve ) and epinephrine stimulate
β1 receptors .
– β1 receptors are G-protein coupled receptors that when activated, stimulate the production of the cAMP .
– Cyclic adenosine monophosphate (cAMP) molecules bind directly to HCN ( funny channels) and increase the number of channels that are open and their permeability to
Na+ , allowing more Na+ to enter.
This speeds the depolarization to threshold and increases heart rate.
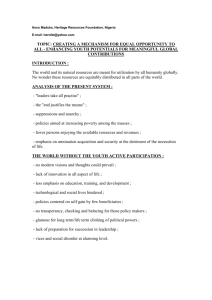
Myocardial Action Potentials cAMP Molecule
Production of Myocardial Action Potentials
• Myocardial cells have a resting membrane potential of ~ -90mV
• Action potentials from pacemaker regions stimulate myocardial cells to depolarize to threshold
– ions such as Na+ and Ca2+ move through gap junctions and raise to threshold.
0. At threshold (-85 MV), fast Voltage-gated Na+ channels open causing a rapid depolarization as Na+ flows into the cell.
1. At ~ +20 mV, fast voltage-gated Na+ channels close and the outward movement of K+ by potassium leak channels brings a brief, small repolarization as the membrane becomes slightly less positive.
2. Slow Voltage-gated (L-type) Ca 2+ channels open allowing Ca 2+ to slowly enter the cell. i. This slight depolarization known as the plateau phase is maintained for 200 to 300 msec before Ca 2+ channels close and complete repolarization happens. ii. The plateau phase results from a slow inward diffusion of Ca2+ through slow voltage gated (L-type) Ca 2+ channels balanced by a slow outward movement (efflux) of K+ through K+ leak channels .
3. Rapid repolarization at the end of the plateau phase is achieved by the closing of the voltage-gated Ca 2+ channels and the opening of voltage-gated K+ channels which causes a rapid outward diffusion of K+.
4. Phase 4 (resting potential): Voltage gated K+ channels close and the permeability’s for sodium, potassium and calcium return to their resting levels.
Electrocardiogram
• Electrocardiogram (ECG or EKG) is a record of the electrical activity conducted through the heart during a cardiac cycle .
– The waves of the ECG are produced by the combined effects of action potentials generated by myocardial cells
–
Each cardiac cycle produces three distinct waves:
1. P wave : Period during which the atria are depolarizing.
–
The spread of an action potential from the SA node through the two atria
2. QRS wave (complex) : The period during which the ventricles are depolarizing, which precedes their contraction.
3. T wave : Period during which the ventricles are repolarizing.
–
Indicates ventricular relaxation and repolarization
Note: There is no wave to show atrial relaxation because the stronger QRS wave masks this event.
6
2. Describe the characteristics and functions of erythrocytes including a description of how
7 oxygen and carbon dioxide are transported. Be sure to include the details of the chloride shift and how RBCs release oxygen at the tissues with emphasis on PO
2
and the Bohr Effect.
Describe the mechanism of clot formation in a damaged blood vessel. Explain how aspirin and plavix work to prevent blood clot formation.
Erythrocytes (Red Blood Cells - RBCs)
• Erythrocytes are round biconcave cells that function to transport oxygen and to a minor extent, carbon dioxide .
– Shape increases surface area for greater gas diffusion.
• Mature RBCs are anucleated and lack mitochondria.
– No nucleus = more room for hemoglobin molecules
– No mitochondria = the RBC will not use the oxygen it is transporting.
•
RBCs generate ATP by anaerobic respiration
• Each erythrocyte contains about 280 million hemoglobin molecules
– A hemoglobin molecule consists of : 4 protein chains called globins and 4 iron containing pigment molecules called heme groups.
• Of the 4 protein chains, 2 are composed of identical alpha chains , and two identical beta chains ,
•
Each protein chain is bound to one heme group
• A heme group consists of a porphyrin ring that holds 1 atom of iron . An iron atom can reversibly bind to one oxygen molecule (O
2
) .
• Hemoglobin gives blood its red color
Carbon Dioxide Transport
• Carbon dioxide is transported in the blood in three forms:
1. As dissolved CO
2 in the plasma, ~10%
2. As carbaminohemoglobin (HbCO
2
) , ~20%. CO
2
is attached to an amino acid in the globin portion.
3. As bicarbonate ion , ~70%
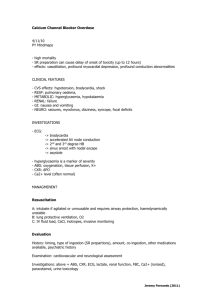
Transport of Bicarbonate Ions and the Chloride Shift
• In order to increase the amount of CO
2
transport,
RBCs convert the CO
2
to bicarbonate and H+ at the systemic capillaries by the following process.
• In systemic capillaries, carbon dioxide combines with water to form carbonic acid, but at a slow rate.
– In RBCs, the enzyme carbonic anhydrase greatly speeds this
reaction to form carbonic acid (H
2
CO
3
).
– As carbonic acid builds up it dissociates into hydrogen ions (H+) and the bicarbonate ions (HCO
3
-) .
• Most of the hydrogen ions (H+) remain in the RBC and attach to hemoglobin (HbH) while most of the bicarbonate ions diffuse out into the plasma by facilitated diffusion and can serve as a buffer .
•
The result is that the inside of the RBC gains a net positive charge .
• This attracts chloride ions (Cl-), which move into the RBCs as HCO
3
- move out . This exchange of anions, diffusion of Cl- into RBCs as HCO3- diffuses out of the RBCs , is called the chloride shift and occurs in the systemic capillaries .
Two factors are involved in the release of oxygen from RBCs at the tissues: PO
2
and the pH
(Bohr Effect)
•
Explains how red blood cells release more oxygen in active tissue.
8
(1) The PO
2
levels. Active tissues use more oxygen causing a decrease in PO
2
of the tissues. The decreased PO
2
of the active tissue results in more O
2
being released from hemoglobin.
• The pH of the tissues and the Bohr
Effect. Active metabolizing tissues release more CO
2
that reacts with water forming carbonic acid . The result is a decrease in pH (increased H+) causing a greater amount of oxygen released from hemoglobin. The unloading of oxygen from oxyhemoglobin is increased by the bonding of H+ (released from carbonic acid) due to a decrease in pH which is known as the Bohr Effect
Reverse Chloride Shift
• In the pulmonary capillaries oxygen binds to deoxyhemoglobin and becomes oxyhemoglobin.
• H+ doesn’t bind well to oxyhemoglobin and H+ is released within RBCs
• The H+ attracts bicarbonate (HCO
3
-) from the plasma, which combines with H+ to form carbonic acid
• Under low CO
2
concentrations, as occurs in the lungs, carbonic anhydrase converts carbonic acid to H
2
O and CO
2
which is exhaled.
Mechanism of Clot Formation in a Damaged Blood Vessel
• Blood loss from a damaged vessel involves three steps: 1) vascular spasm 2) formation of a platelet plug, and 3) clot formation
– production of a of a fibrin web.
1) Vascular spasm :
– A cut or torn vessel immediately constricts and reduces blood flow through the vessel.
2) Formation of a platelet plug :
– Breakage of the endothelial lining of a vessel exposes collagen fibers from the basement membrane of the endothelium.
9
– Collagen fibers activate platelets to change shape (spiky processes) and become sticky which causes them to bind with the collagen fibers and other platelets to form a platelet plug .
– Endothelial cells in the injured area produce a protein called von Willebrand’s factor which binds to both collagen and platelets holding them together .
– Activated platelets release several chemicals from their storage granules including adenosine diphosphate (ADP) and thromboxane A
2
(TxA
2
) . Both of which activate other platelets.
– Thromboxane A
2
(a prostaglandin) is also a powerful vasoconstrictor which reinforces vascular spasms .
– Platelets also release chemicals to stimulate fibrin formation in the blood clot.
3) Clot Formation - production of a fibrin web : Blood clotting is the transformation of blood from a liquid into a solid structure that strengthens the platelet plug.
– The final step in clot formation is the conversion of fibrinogen , a soluble protein produced by the liver and normally present in the blood to fibrin , an insoluble threadlike molecule. Actually fibrin monomers attach to produce a fibrin polymer.
• Fibrin molecules adhere to the damaged blood vessels surface forming a netlike meshwork that traps blood cells – the resulting mass of platelets, blood cells, and fibrin becomes the blood clot.
– Thrombin is the enzyme that converts fibrinogen to fibrin at the injury site.
• Prothrombin, produced by the liver and normally present in the blood, is the inactive form of thrombin
•
Prothrombin i s converted to thrombin by factor X (prothrombinase), which was activated by a cascade of a number of clotting factors including thromboplastin and Ca 2+ .
Blood Clot Prevention - Aspirin and Plavix
• Thromboxane A
2 is a prostaglandin required for platelet aggregation and is a potent vasoconstrictor . The formation of thromboxane A
2
is catalyzed by the cyclooxygenase-1
( COX-1) enzyme .
– Aspirin is a COX-1 and COX-2 inhibitor and thus reduces platelet aggregation by inhibiting thromboxane A
2
production.
– Since platelets are not compete cells, they cannot regenerate new enzymes and thus the COX-1 enzyme is inhibited for the life of the platelet (~10 days). Note: aspirin can significantly increase bleeding times.
• Plavix inhibits platelet activation by blocking the receptors for ADP on the platelet plasma membrane.
3. Using a diagram, provide an overview of the main factors that determine mean arterial
10 pressure. Be sure to include arrows and do not abbreviate words in the graph. Explain how the kidneys regulate blood volume and be sure to include details about antidiuretic hormone
(ADH, vasopressin), aldosterone, and the rennin-angiotensin-aldosterone system. Explain how
ACE Inhibitors work. Describe what circulatory shock is and explain the four main types.
Define Edema and describe the 5 primary causes of edema.
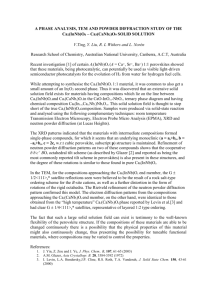
Overview of the main factors that determine of Mean Arterial Pressure
Regulation of Blood Volume by the Kidneys
• The kidneys produce ~180 L (50 gal) per day of blood filtrate.
– ~98% of the filtrate is reabsorbed back into the vascular system.
– ~1.5 L of urine is excreted per day.
• Hormones that regulate blood volume in the kidney include:
– Antidiuretic Hormone (ADH)
– Aldosterone
– Renin-Angiotensin-Aldosterone System
Antidiuretic Hormone (ADH)
• Antidiuretic hormone (ADH)
– Synthesized by the hypothalamus and released by the posterior lobe of the pituitary gland
– Acts to increase blood volume and pressure
– Released in response to increased plasma concentrations
( osmolality ) that can be due to dehydration or by excessive salt intake.
• Stimulation of osmoreceptors produces sensations of thirst and increased water intake, which increases blood volume.
• ADH stimulates water reabsorption from the kidney filtrate and thus a smaller volume of urine is excreted and maintains blood volume.
Regulation of Blood Volume by Aldosterone
• Aldosterone : Stimulates kidneys to reabsorb salt (specifically Na+).
–
Retention of salt causes an increase in water reabsorption.
• Aldosterone increases blood volume, but, unlike ADH, it does not produce a change in plasma osmolality because salt and water are reabsorbed in proportional amounts.
– A “salt-retaining hormone”
• Aldosterone secretion (by adrenal cortex) is stimulated by the Renin-Angiotension-
Aldosterone System which is responsive to:
– Decreased Na+ concentrations
–
Reduced blood volume and pressure
11
Renin-Angiotensin-Aldosterone System Mechanism of Action
• Steps in this magnificent process
1. Decrease in blood pressure (BP) and/or a decrease in Na+ concentration is sensed by specialized cells of the juxtaglomerular apparatus .
• Juxtaglomerular apparatus contains:
• Macula densa cells located at the top of the ascending limb of the renal tubule.
• Function to monitor Na+ concentration of tubular filtrate.
• Juxtaglomerular cells are modified smooth muscle cells located in the wall of the afferent arteriole.
• Function as baroreceptors to sense changes in blood volume or pressure and secrete the enzyme renin .
12
• Juxtaglomerular cells , in communication with the macula densa cells , release renin into the blood in response to a decrease in blood pressure, blood volume and/or a decrease in Na+ concentration.
2. Renin enters the blood stream and converts the protein angiotensinogen to angiotensin I.
3. Angiotensin I is converted to angiotensin II by an angiotension-converting enzyme
(ACE) as it passes through the capillaries of the lungs.
4. Angiotensin II causes blood pressure and volume to rise by the following:
• For Increased Blood Pressure:
• Is a powerful vasoconstrictor of small arteries and arterioles which increases total peripheral resistance and increases arterial BP
• For increased blood volume (and thus BP):
• Stimulates the adrenal cortex to release aldosterone , a hormone that promotes Na+ and water retention at the kidneys and thus increases blood volume and BP
• Stimulates ADH release by the posterior pituitary which increases blood volume and thus BP
• Activates the body’s thirst center within the hypothalamus ;
• Thirsty person drinks more - increased fluid intake causes an increase in blood volume and BP
5. High salt intake , leading to high blood volume and pressure, inhibits renin secretion .
• Less aldosterone means less salt is retained by the kidneys and more is excreted in the urine.
Clinical Application: ACE Inhibitors
• Hypertension (high blood pressure) can be treated with angiotensin converting enzyme
(ACE) inhibitors .
– Block the formation of Angiotensin II , thus reducing its vasoconstrictor effect.
– Increase activity of bradykinin, a chemical that promotes vasodilation which decreases total peripheral resistance (TPR).
• Good for treatment of congestive heart failure since TPR is decreased.
Circulatory Shock
•
Circulatory shock occurs when blood pressure falls so low that adequate blood flow to the tissues can no longer be maintained, especially to the brain
• Four main types:
1.
Hypovolemic (“low volume”) shock
• Caused by severe hemorrhage or through loss of fluids (severe diarrhea, excessive urination, extensive sweating)
2.
Cardiogenic (“heart produced”) shock
• Weakened heart’s failure to pump blood adequately
3. Vasogenic (“vessel produced”) shock
• Widespread vasodilation triggered by vasodilator substances – two types:
• Septic shock: Massive infection - infectant releases vasodilator substances.
• Anaphylactic shock: Extensive histamine release is severe allergic reactions.
4. Neurogenic (“nerve produced”) shock
• Loss of sympathetic vascular tone leads to generalized vasodilation.
– Can be caused by damage to central nervous system or excruciating pain.
13
Edema
• Edema: Excessive accumulation of interstitial fluid.
– Disturbance in the capillary and/or problems with lymphatic drainage.
• Causes of Edema.
– High arterial pressure : Increases capillary pressure and causes excessive filtration.
• Hypertension
– Increased venous pressure : Produces a congestive increase in capillary pressure
• Thrombosis (thrombus forms in a vein)
• Pregnancy (mechanical compression of veins)
• Varicose veins (blood pulls in veins)
•
Congestive heart failure
– Decreased plasma protein concentration : Less capillary colloid osmotic pressure to pull fluid back in.
• Liver disease (decrease in albumin production)
• Kidney disease (excessive loss of proteins in urine)
• Starvation (decrease in ablumin production)
• In children, fluid accumulates in the abdominopelvic cavity, producing the swollen bellies typical of starvation victims.
– Increased capillary permeability allows leakage of plasma proteins into the interstitial fluid : Less colloid osmotic capillary pressure to pull fluid back in.
• Tissue injury or allergic reactions (histamine increase capillary permeability)
– Obstruction of lymphatic drainage : Prevents return of excess interstitial fluid
• Filariasis: Filaria roundworm infection
– transmitted by mosquito.
• Elephantiasis
• Roundworms block lymphatic drainage