The Nelson Health Centre Direct Access Cardiac Diagnostics
advertisement

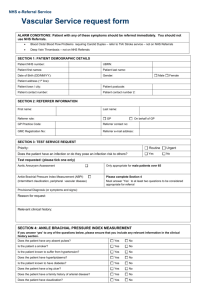
The Nelson Health Centre Direct Access Cardiac Diagnostics Referral Form If this form does not contain all the required information, it will be returned. Fax no. 020 8725 4215 Email nelson.referrals@stgeorges.nhs.uk Forename: DOB: M□ F□ Surname: Address GP details: NHS no. Email: Tel Referral Date: Medical History / Risk Factor: Existing IHD Smoking HX Diabetes Hypertension Hyperlipidaemia □ □ □ □ □ Family HX □ Diagnostic Test Request: Please tick tests required: ECG□ 24 ECG Monitor □ 48 ECG Monitor □ 72 ECG Monitor □ BP monitor □ Event Recorder □ Exercise Test □ Echo □ Please note: All cardiac investigations that are deemed to be normal will be sent back to referrer with a cardiac physiologist’s report only. Abnormal investigations will be reviewed by cardiologists and a report sent back to the referrer with clinical recommendations. If you wish to refer for a cardiology consultation please refer using the generic referral form. Please add any relevant information: Signature of Referrer ________ Excellence in specialist and community healthcare Date ______