Vascular Service Request Form (Opens in a new window)
advertisement
")
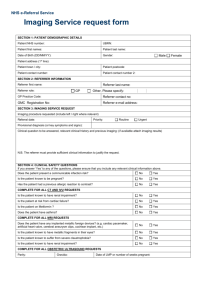
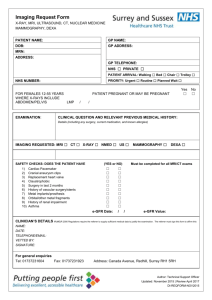
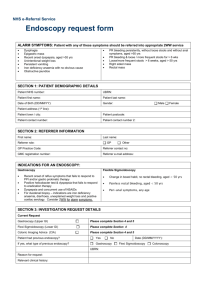
NHS e-Referral Service Vascular Service request form ALARM CONDITIONS: Patient with any of these symptoms should be referred immediately. You should not use NHS Referrals. Blood Clots/ Blood Flow Problems requiring Carotid Duplex – refer to TIA/ Stroke service – not on NHS Referrals Deep Vein Thrombosis – not on NHS Referrals SECTION 1: PATIENT DEMOGRAPHIC DETAILS Patient NHS number: UBRN: Patient first names: Patient last name: Date of Birth (DD/MM/YY): Gender: Male Female st Patient address (1 line): Patient town / city: Patient postcode: Patient contact number: Patient contact number 2: SECTION 2: REFERRER INFORMATION First name: Referrer role: Last name: GP On behalf of GP GP Practice Code: Referrer contact no: GMC Registration No: Referrer e-mail address: SECTION 3: TEST SERVICE REQUEST Priority: Routine Urgent Does the patient have an infection or do they pose an infection risk to others? Yes No Test requested: (please tick one only) Aortic Aneurysm Assessment Only appropriate for male patients over 65 Ankle Brachial Pressure Index Measurement (ABPI) Please complete Section 4 (Intermittent claudication, peripheral vascular disease) Must answer ‘Yes’ to at least two questions to be considered appropriate for referral Provisional Diagnosis (or symptoms and signs): Reason for request: Relevant clinical history: SECTION 4: ANKLE BRACHIAL PRESSURE INDEX MEASUREMENT If you answer ‘yes’ to any of the questions below, please ensure that you include any relevant information in the clinical history section. Does the patient have any absent pulses? Yes No Is the patient a smoker? Yes No Is the patient known to suffer from hypertension? Yes No Does the patient have hyperlipidaema? Yes No Is the patient known to have diabetes? Yes No Does the patient have a leg ulcer? Yes No Does the patient have a family history of arterial disease? Yes No Does the patient have claudication? Yes No