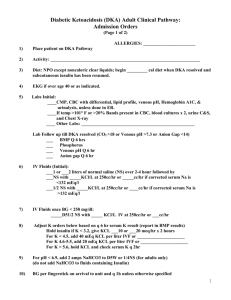
Diabetes and Blood Glucose Emergencies
advertisement

(+)CoreyM.Slovis,MD,FACEP Professor,EmergencyMedicineandMedicine; Chairman,DepartmentofEmergencyMedicine, VanderbiltUniversityMedicalCenter,Nashville, Tennessee;MedicalDirector,MetroNashvilleFire DepartmentandNashvilleInternationalAirport AdvancedPracticeProvider Academy April14‐18 SanDiego,CA DiabetesandBloodGlucoseEmergencies:How SweetItIs! Diabetesandderangementsofbloodglucosemetabolism representsasignificantnumberoftrueemergenciesas wellashasanimpactonavastnumberofpatientswho presenttotheemergencydepartment.Hyperglycemicand hypoglycemicstatesarenotonlylife‐threateningbutcan mimicothercriticalpathologicconditionsandneedtobe identifiedandmanagedquickly.Thiscoursewill introduceapproachestotheidentificationand managementofpatientswithbloodglucoseemergencies, diabeticketoacidosis(DKA)andhyperglycemic hyperosmolarsyndrome(HHS)—andthecontroversy thatsurroundsthemanagementofthesediseases.The extremeoppositeoftheaboveprocessesandthecauses andmanagementofhypoglycemicstatesalsowillbe discussed. Objectives: Identifypatientswhohavebloodglucose derangementsandreviewsomecommonconditions thattheymimic. Describethecommonpresentation,laboratory abnormalities,treatmentandadmissioncriteriafor patientswithdiabeticemergencies. Discusscurrentdifferencesbetweentheapproachto adultsandpediatricpatientswithhypoglycemia. Date:4/14/2014 Time:2:45PM‐3:15PM CourseNumber:MO‐12 (+)Nosignificantfinancialrelationshipstodisclose DKA, HONK, Hypoglycemia DKA Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN Mastering Emergency Medicine A 21 year old grad student Presents in DKA. How many causes of DKA are there? 5 Causes of DKA • Secure the ABC’s • Consider or give NGT • Five Causes • Five Steps • Five Reasons for almost everything DKA – Insulin Lack 5 Actions of Insulin • Infection • Drive Glucose into cell → Glu ↑ • Infarction • Drive K into cell →K↑ • Infant • Anabolic → Catabolic • Indiscretion • Block Fat breakdown → FFA Acids ↑ • Insulin lack • Block protein breakdown → Keto Acids ↑ 1 Diabetes Care 2009;32:1335-1343 How Sick in DKA? • Mental Status • BP/Pulse • Current State of the Art • Respiratory Rate • Standard of Care • Finger Stick Glucose • Consensus Statement of ADA • Venous pH Three Levels of DKA Mild pH pH in DKA Moderate 7.25 – 7.30 7.00 – 7.24 Severe below 7.0 HCO3 15 - 18 10 - 15 below 10 MS Alert Alert + Stupor or Coma • Which is better, an ABG with arterial pH or just a venous pH? Acad Emerg Med 2003;10:8 Routinely Use VpH in DKA. • 200 ABGs and VpHs in DKA Patients • ABG pO2 and pCO2 changed Rx in 2/200 • Very high correlation between Art pH vs. V pH (0.95) 2 Five Therapies to Consider in DKA How many therapies should you consider in DKA? • Volume v• Insulin • Potassium ...................... • Bicarbonate • Phosphate Therapy and Rationales in DKA • Volume – Enough to re-hydrate – But don’t wash out ketones • Insulin – Saturate receptors – And keep saturated • Potassium – Avoid hyperkalemia early – But avoid hypokalemia later Therapy and Rationales in DKA - 2 • Bicarbonate – Rarely needed – Use for decompensation • Phosphate – Only cachectic adult patients – Common in children – Use for values below 1.0 – 1.5 VOLUME in DKA Deficits: • 3 - 5 liters is usual deficit in mild-moderate DKA What is the best IV flow rate in DKA for the first 3 to 4 hours? • 5 - 6 liters is usual fluid deficit in severe DKA 3 JAMA 1989;262:2108-13 Don’t “wash out” all the Keto Acids …. Let the Patient Metabolize Them Volume Therapy in DKA Begin Therapy: • Bolus healthy patients with at least 1,000 cc of NSS (20 cc/kg) rapidly Stable Patients: • NSS at 500 cc/hr x 4 hours • Switch to NSS at 250 cc/hour For Mild DKA You Can Just Begin Therapy at 250cc/hr with Smaller or no Bolus. Profound Dehydration: • NSS wide open until well perfused NSS vs. ½ NS • NSS is the “standard” • Use initially to volume load • Consider ½ NS if corrected serum sodium is elevated 4 The easiest way to correct for Na in DKA is 2-2.5 meq ↓ Na for every 100mg/dl ↑ glucose “Real Formula” – 1.6 ↓ Na/100 ↑ mg/dl glucose to 400 4.0 ↓ Na/100 ↑ mg/dl > 400 Once Serum Glucose approaches 250 mg%: Switch to Glucose containing fluids (D51/2 NS at 150 - 250 cc/hr) Cerebral Edema and DKA • Seen in children • Increased morbidity and mortality • Leading cause of death in pediatric DKA NEJM 2001;344:264-269 The only therapeutic variable associated with cerebral edema in children with DKA was the administration of Bicarbonate. • Lower pH and pCO2 increases incidence • Aggressive fluids also implicated • Low pH, low pCO2 levels and amount of dehydration also important Fluids in DKA • Bolus: adults routinely, children rarely • Correct hypoperfusion ASAP • Less, not more, once euvolemic Children are at Real Risk for Cerebral Edema. Be Careful! • Under-resuscitation is to be avoided • Acidosis and Dehydration are your enemies 5 Insulin Insulin Dosing You must: • Provide a loading dose, and then • Keep all receptor sites saturated Each unit of insulin moves about 4-5 grams of glucose into cell. • Loading Dose – 0.1 units/kg IV Push • Maintenance Dose – 0.1 units/kg per hour In general load adults, not children J Emerg Med 2010;38:422-427 • ADA recommends insulin loading in adults • Loading dose saturates receptors J Emerg Med 2010;38:422-427 Conclusions • IV insulin bolus not of proven benefit • Loading may cause hypoglycemia in children • Loading not recommended in Peds DKA • May cause more hypoglycemia Potassium in DKA If glucose fall is not at 100 mg/dl per hour, rebolus, double infusion rate and look again for infection, infarction and infant. • The average K deficit in DKA is 3 - 5 meq/kg IBW • The ECG does not accurately predict hypokalemia 6 Potassium Dosing in DKA A patient in DKA presents with K=5.1, pH =7.0, good urine output. How much KCl should be given in the first 4 hours? In general 10 meq/hr But … KCL Replacement in First Hours of DKA Be sure K is in the DKA range of WNL. 4.0 - 5.3 Hyperkalemia (above 5.3) Hold K for 1 hr, recheck K “DKA Kalemia” (4.0 - 5.3) KCL 10 meq/hr Hypokalemia (3.5 - 4.0) KCL 20 meq/hr Severe HypoK (below 3.5) Hold Insulin KCL 20 - 60 meq/hr/constant ECG Unexpected Death in DKA • First hour or two when sick: – Hyperkalemia • Later while “stabilizing”: A patient is treated for DKA and his glucose falls appropriately. His bicarbonate however, does not rise. First thoughts? – Hypokalemia 7 Refractory Acidosis in DKA • Dead Gut • Sepsis • Abscess Recommendations on Bicarbonate Bicarbonate Use Potential Benefits Potential Risks Reverses Acidosis Intracellular Acidosis Improves Cardiac Output Increased Ca, H+, K fluxes Increases Fibrillatory Threshold Hypokalemia, Tissue Hypoxia Improves Insulin Sensitivity Hyperosmolarity, Hypernatremia Decreased Work of Breathing Increased CO2 Generation, Respiratory Acidosis Decreased Length of Coma Paradoxical CSF Acidosis HCO3 PCO2 pH 24 40 7.40 20 35 7.35 15 30 7.30 • pH between 6.9 - 7.0 may require bicarbonate 10 25 7.25 5 15 7.12 • pH below 6.9 probably requires bicarbonate 2.5 15 6.88 It is generally agreed that: • pH above 7.0 requires NO bicarbonate If you give HCO3 rapidly IV: • Serum HCO3 will rise Rapid IV administration of bicarbonate in DKA can cause a respiratory acidosis in the brain • Thus serum pH will rise • If pH rises, less hyperventilation • Serum pCO2 will rise on venous side • Causing pCO2 to rise on CSF side too 8 Is Bicarbonate Really Hyperosmolar? N Engl J Med 2001;344:264-9 • Osmolarity = 2 x Na + Glu/18 + BUN/2.8 • Na is in meq/L • Na HCO3 = 1 meq/ml or 1000 meq/L • Osm Na HCO3 = 2 x 1000 = 2000 mOsm! Push Bicarb ONLY For: • Hyperkalemic emergency Phosphate Therapy in DKA • Impending cardiopulmonary arrest Phosphate Therapy in DKA • No proven benefit • Rarely used in adults NKHC, HONK • Up to ½ of K requirements given as K2 PO4 in pediatric patients. • Check with your pediatrician 9 5 Actions of Insulin • Drive Glucose into cell → Glu ↑ Nonketotic Hyperosmolar Coma (NKHC, HONK) • Not enough insulin to move glucose • Drive K into cell →K↑ • Anabolic → Catabolic • Enough insulin to block catabolic state • Block Fat breakdown → FFA ↑ • Enough to not breakdown fat & protein • Block protein breakdown → Keto Acids ↑ Nonketotic Hyperosmolar Coma (NKHC) Insulin levels Ketoacidosis Glucose HCO3 OSM Age Onset Associated diseases Seizures Coma Mortality DKA very low profound 600 5 300 - 325 young acute rare very rare rare approaches 0 NKHC may be normal minimal 1,000 20 - 24 350+ old chronic common common common 20 - 40% NKHC/HONK • Volume resuscitate NSS • Slow fluids to 200-250cc/hr • Use NSS if corrected Na < 135 • Use ½ NSS if Na corrects > 135 • Enough insulin to drive K into cell • Extreme glucose elevations NKHC • AMS in most patients • Up to 50% present in deep coma • Seizures in up to 1/4 of patients • Often focal (20 - 85% of reported cases) • Patients usually lethargic or comatose • 10% present without AMS Insulin in NKHC • ADA guidelines recommend bolus and maintenance like in DKA • 0.1 units/kg bolus and 0.1 units/kg per hour • My bias, go slower • KCI at about 10meq/hr 10 • It takes hours to 1-2 days to develop DKA –Treat aggressively • It takes many days to weeks to develop NKHC – Do not treat aggressively Hypoglycemia Hypoglycemia ReExPLAIND Re Ex P L A I N D Renal Exogenous Insulin/antihyperglycemics Pituitary Insufficiency Liver Alcohol, Addison’s, Aspirin Infection, Insulinoma Neoplasm Drugs Treating NKHC • Twice the volume deficit, but Treat ½ as aggressively as DKA • Tease with insulin, no drip • DKA pts should never die, NKHC often do Why does every hypoglycemic patient’s low blood glucose have to be ReExplained? Hypoglycemia (Renal) • Decreased insulinase • Decreased excretion • Decreased caloric intake • Increased number of infection 11 Hypoglycemia (Drugs) • Beta Blockers • Alcohol • Aspirin • Pentamidine One amp of D50 should raise serum glucose by about 200 mg/dl for up to 30 minutes. If it doesn’t look for complicating factors like sepsis, insulin OD, oral agent OD, or ASA OD • Valproic Acid One Amp of D50 • 50% Dextrose in Water • 50 cc of 50% = 25 grams • 100 calories Dextrose does not last too long reliably, But in first 5-10 minutes will raise glucose by about 200 mg% • Lasts 5-30 minutes reliably • After 30 minutes: feed or D5W D50 Mistakes • Not needed Glucose Dosing • Adult D50 1 cc/kg • No secure IV line • Child D25 2 cc/kg • Pushed too quickly • Neonate D10 2-4 cc/kg • Repeated too quickly • Given in too young a patient 12 Hypoglycemic But No IV Ann Emerg Med 1991;20:375-379 • Oral Glucose Gel • • • • • • Glucagon IM Ann Emerg Med 2000;36:133-138 • Decreased Hypoglycemic episodes by a factor of 27 • D50 rarely required post octreotide • Stabilization was immediate Glucagon stimulates cAMP and block insulin Can be given IM if no IV available 1.0 mg IM will elevate glucose about 100 mg% Onset of action is 5-15 minutes Effective 50-98% of the time The signs and symptoms of hypoglycemia are variable and are dependent on both: – Low Glucose Levels – Rate of Fall of Glucose Always Check Glucose Nobody dies of hyperglycemia They do from Hypoglycemia • AMS • Seizures • Post-ictal • CVA • Weak, Dizzy 13 Therapy and Rationales in DKA • Volume Summary – Enough to re-hydrate – But don’t wash out ketones • Insulin – Saturate receptors – And keep saturated • Potassium – Avoid hyperkalemia early – But avoid hypokalemia later Therapy and Rationales in DKA - 2 Volume Therapy in DKA Begin Therapy: • Bicarbonate – Rarely needed – Use for decompensation • Phosphate – Only cachectic patients – Use for values below 1.0 – 1.5 Refractory Acidosis in DKA • Dead Gut • Bolus healthy patients with at least 1,000 cc of NSS (20 cc/kg) rapidly Stable Patients: • NSS at 500 cc/hr x 4 hours • Switch to NSS at 250 cc/hour Profound Dehydration: • NSS wide open until well perfused NKHC/HONK • Volume resuscitate NSS • Slow fluids to 200-250cc/hr • Sepsis • Use NSS if corrected Na < 135 • Abscess • Use ½ NSS if Na corrects > 135 • KCI at about 10meq/hr 14 Hypoglycemia ReExPLAIND Re Ex P L A I N D Renal Exogenous Insulin/antihyperglycemics Pituitary Insufficiency Liver Alcohol, Addison’s, Aspirin Infection, Insulinoma Neoplasm Drugs Summary • DKA - fluid bolus - NSS, insulin, K • Beware Hypokalemia in DKA • Go slow in HONK • Re-explained all hypoglycemia • Check glucose 15