Prolonged Neonatal Jaundice Protocol
advertisement

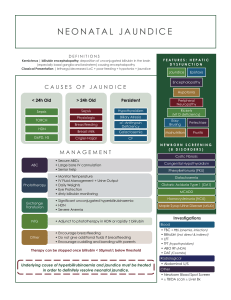
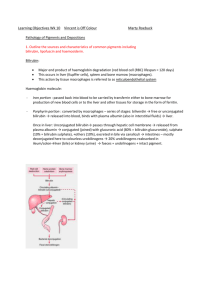
Paediatric Protocol Gastrointestinal: 11.3 January 2001 Prolonged Neonatal Jaundice Protocol As jaundice is present in up to 90% of newborn babies, liver disease may be difficult to detect. In practice, if jaundice persists beyond two weeks after birth it should be investigated even in breast-fed babies. In a well child, the first step is to examine the stools and urine. If the stools are pale and the urine contains bilirubin, the child needs urgent referral to a Paediatric Gastroenterologist to exclude biliary atresia etc. The second step is to confirm whether the prolonged jaundice is due to an elevation of conjugated or unconjugated bilirubin in the plasma (split bilirubin). See Summary Flow chart Unconjugated Hyperbilirubinaemia If the estimation of bilirubin indicates that > 85% is unconjugated, then breast milk jaundice or another cause of unconjugated hyperbilirubinaemia is likely (Table 1). Appropriate further investigations should include: 1. 2. 3. 4. 5. H a e m o l y s i s Full blood count, including reticulocytes Examination of blood film Thyroid function tests Gal-1-Put – i.e. red cell galactose-1-phosphate uridyl transferase Urine culture Table 1. Causes of unconjugated hyperbilirubinaemia Breast Milk Jaundice Haemolysis Blood group incompatibilities (ABO & Rhesus) Polycythaemia Extravasated Blood Increased Enterohepatic Circulation Pyloric stenosis Bowel obstruction Endocrine/Metabolic (also cause conjugated hyperbilirubinaemia) Hypothyroidism Hypopituitarism Hypoadrenalism Galactosaemia Sepsis January 2001 Page 1 of 4 Dr David Bond Conjugated Hyperbilirubinaemia If > 15% of the total bilirubin is conjugated or bilirubin is detected in the urine, liver disease must be excluded. The differential diagnosis is extensive (Table 2), but it is essential to exclude biliary atresia early by examining the stools and urine. If the stool is pigmented, coagulation needs checking, and further investigations should be coordinated by a Paediatric Gastroenterologist looking for causes of neonatal hepatitis. The key is to arrange a HIDA scan, which should only be performed after five days of oral Phenobarbitone (5mg/kg/day). This gives sufficient time for the following tests to be performed: 1. Liver function tests 2. Coagulation screen 3. Blood glucose 4. Full blood count 5. TORCH screen / Hepatitis serology 6. Alpha-1-Antitrypsin level and phenotype (Li. Hep.) or genotype (EDTA) 7. Gal-1-Put 8. Thyroid Function Tests 9. Random Cortisol 10. Plasma amino acids 11. Serum iron and ferritin 12. Urine culture 13. Urine metabolic screen Immediate referral to a Paediatric Gastroenterologist is mandatory if a neonate has two or more of the following: Conjugated hyperbilirubinaemia > 40 mol/l Pale stools Bilirubin in urine Bleeding tendency Failure to thrive Recurrent hypoglycaemia More specialized investigations will include: 1. HIDA Scan after enzyme induction for five days with Phenobarbitone (5mg/kg/day in a single dose) 2. Abdominal Ultrasound 3. CxR (butterfly vertebrae) 4. Eye examination (posterior embryotoxin) 5. Liver biopsy (after correction of coagulopathy) 6. Echocardiography (pulmonary stenosis) 7. Sweat test January 2001 Page 2 of 4 Dr David Bond Contact Dr Charlton at Queen’s Medical Centre (Secretary on 42439 or Page via switchboard). In Dr Charlton’s absence, infants should be referred to the Paediatric Liver Unit at St.James’ Hospital, Leeds. Table 2. Causes of conjugated hyperbilirubinaemia A. Extrahepatic biliary duct disorders Biliary atresia Choledochal cyst Gallstone B. Bile Duct Hypoplasia Syndromes (Alagilles) C. Neonatal Hepatitis Syndrome Idiopathic Neonatal Hepatitis Syndrome Intrauterine Infections Metabolic Hypothyroidism Hypopituitarism -1 antitrypsin deficiency Galactosaemia Tyrosinaemia Type 1 Hereditary fructose intolerance Niemann Pick Type C Zellweger’s Cystic fibrosis Sepsis Urinary Tract infection Sepsis Urinary tract infection Prolonged parenteral nutrition January 2001 Page 3 of 4 Dr David Bond Flow Chart For Management of Prolonged Neonatal Jaundice Jaundiced infant > 2 weeks old Stools pale and NO bilirubinuria YES Initial Investigations: LFT with split bilirubin FBC + Reticulocytes TFT Gal-1-Put Urine culture Urgent referral to Paediatric Gastroenterologist Unconjugated bilirubin Conjugated bilirubin > 85 % of total > 15 % of total Registrar to chase results and ensure formal GP letter written References 1. Ives N K. Neonatal Jaundice. Current Paediatrics (1997) 7, 67-72. 2. Kelly D A. Hepatology in Investigations in Paediatrics. Addy and Douglas (eds.) (1994) 123-130. WB Saunders. 3. Roberts, E A. The Jaundiced baby in Diseases of the Liver and Biliary System in Children. Kelly (ed) (1999) 11-45. Blackwell Science. January 2001 Page 4 of 4 Dr David Bond