Urine sample form
advertisement

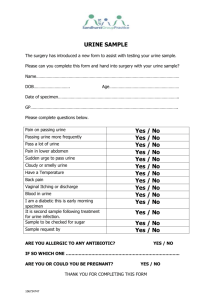
URINE SAMPLE If under 12 years of age – SEE GP unless otherwise advised Note: URINE SAMPLES are very difficult to interpret without this information NAME……………………………………………………………………………….. DOB……………………………… TODAYS DATE and TIME of SAMPLE TAKEN………………./…………………/2015. PLEASE CIRCLE ANSWER ARE YOU DIABETIC? ARE YOU PREGNANT? DO YOU HAVE A CATHETER? ………………………..AM/PM YES/NO YES/NO YES/NO F YOU THINK YOU HAVE AN INFECTION PLEASE TICK THE FOLLOWING SYMPTOMS WHICH APPLY PAIN WHEN PASSING URINE GOING MORE OFTEN/URGENCY FEVERISH BACK and/or LOWER ABDOMINAL PAIN FEEL UNWELL OTHER – give details………………………………………………………………………………………………… Can we e-mail back the result (please supply e-mail address) YES/NO …………………………………………………………………………………………………. or contact you by mobile (please supply current mobile number) YES/NO ……………………………………………………………………………………………….. Or land line (please supply current land line number) YES/NO ……………………………………………………………………………………………….. Can we leave a message Editor: JMLP/My Docs/Mastercopies/Urine January 2015 YES/NO