Ischemic Colitis
advertisement

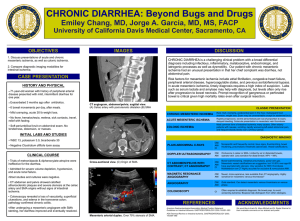
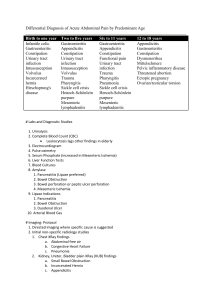
ISCHEMIC COLITIS Pablo Quintero Pinzon August,2005 General description Ischemic colitis is the most common cause of gastrointestinal ischemia (50-60%), followed by acute mesenteric ischemia (30-40%), focal segmental ischemia (5%), and chronic mesenteric ischemia (<5%). It is most often has a non-occlusive mechanism, and results in the shunting of blood away from the bowel mucosa. The actual pathophysiology of the ischemia is likely related to bowel hypoxia and lack of nutrients necessary for cellular metabolism and integrity. It can occur acutely or chronically and secondary to a variety of mechanisms. Anatomy Superior Mesenteric Artery (SMA) Supplies ascending and proximal transverse colon Arises from the aorta at L1 Inferior Mesenteric Artery (IMA) Supplies the distal transverse colon and descending colon Arises from the aorta at L3 Internal Iliac Hypogastric Arteries Supplies the rectum via the middle and inferior rectal/hemorrhoidal arteries Watershed areas Superior rectum (between IMA and celiac beds) Transverse and left sided colon (between IMA and SMA). Griffith’s point is the tenuous area between the SMA and IMA near the splenic flexure. Causes Most often, no specific cause is identified. Incidence increases with age (<70 years), DM, HTN, CAD, and smoking, perhaps because of worsening atherosclerotic disease. Occlusive IMA thrombosis Arterial/cholesterol embolus: arrhythmias with risk of emboli into the vascular supply (i.e. afib) Iatrogenic: s/p aortoiliac vascular reconstruction, AAA repair, abdominoperineal resection with sacrifice of IMA Mechanical obstruction: adhesions, volvulus, carcinoma, stricture Localized low flow: vasculitis, hematologic diseases (sickle-cell, protein c/s, AT III), parasitic infxn (usually affect watershed areas) Non-occlusive disease Systemic low-flow states: CHF, dig toxicity, cardiac dysrhythmia, shock, MI (usually R. colon) Medication related: estrogen, danazol, vasopressin, gold, psychotropic drugs, sumatriptan Clinical Features Acute Most cases are more mild and may present with bloody stools without abdominal pain Some present with severe, crampy lower abdominal pain, rectal bleeding, and hypotension Also may have fever and elevated white count In severe cases, may see colonic dilation and physical signs of peritonitis (transmural infarction) and perforation Beth Israel Deaconess Medical Center Residents’ Report Subacute Lesser degree of pain and bleeding that may occur over days to weeks Lower rectum is usually spared because of collateral blood supply Most resolve in 2-4 weeks and do not recur (approximately 50%) Stricture formation may result from ischemia if the muscularis is involved in the ischemic insult. If stricture formation occurs, surgery may be required to repair the stricture. Diagnosis Diagnosis usually stablished based upon clinical setting, physical examination and radiologic and/or endoscopic studies. Labs may show elevated white count, lactic acidosis, elevated LDH, phosphate, CPK, amylase. WBC >20.000 and metabolic acidosis may indicate gangrenous necrosis. Stool cultures should be ordered except in patients who developed the symptoms more than 72 hours after being admitted to the hospital. Imaging may reveal thumbprinting (on plain films) or thickening of the bowel wall in a segmental pattern (on CT), caused by submucosal edema and bleeding. Thumbprinting disappears within days. Distension or neumatosis are typically seen only in advanced ischemia. Direct visualization with sigmoidoscopy and/or colonoscopy may show mucosal ulcerations, friability, and bulging folds from submucosal edema/bleeding. Should only be attempted in patients with no signs of peritonitis and normal plain films. Insufflation to greater than 30 mm Hg may lead to worsened ischemia. Biopsy may show submucosal hemorrhage, crypt destruction, sloughing of epithelial cells, and capillary thrombosis. Histology may reveal mucosal infarction or ghost cells. Angiography is rarely useful because remediable occlusive lesions are rarely found. In most cases colonic blood flow has returned to normal by the time of symptom onset, therefore, angiography will be normal. However, may be indicated when acute mesenteric ischemia (defined as ischemia of all or part of the small bowel and ascending colon) is considered or when the patient has more severe abdominal pain. Laparoscopy may be an important dx tool specially in the elderly who may tolerate laparotomy poorly. Limitation- only visualizes the serosal surface of the gut which may be normal initially. Magnetic Resonance Angiography, not a lot of data. Might be useful for preoperative assessment of the proximal mesenteric artery and evaluation of portal hypertension. Differential Diagnosis Usually distinguished by colonoscopy or sigmoidoscopy in absence of peritoneal signs or significant abdominal pain and with stool studies. Inflammatory bowel disease Diverticulitis Infectious colitis Colonic malignancy Treatment Medical management Maintain hemodynamic stability using iv hydration, optimizing cardiac output Keep NPO. NG tube if ileous present. Prophylactic antibiotics may be indicated if evidence of peritonitis or translocation of bacteria across the bowel wall Close monitoring with abdominal films, serial exams to look for perforation or obstruction. Monitor wbc, hct, electrolytes Avoid medications that may restrict intestinal bloodflow (sumatriptan, octreotide) Beth Israel Deaconess Medical Center Residents’ Report Surgical management Necessary when clinical deterioration despite conservative therapy. When colonic infarction has occurred Prognosis Difficult to predict unless intraabdominal catastrophe is obvious. Most patients with nonoclussive ischemia improve after 24-48 hours, and have completely clinical and radiological resolution within 1 to 2 weeks Approximately 50% have reversible damage and the other half develop gangrene (15-20%), chronic, segmental ulcerating colitis (20-25%), stricture (10-15%), or fulminant colitis (1-2%). Beth Israel Deaconess Medical Center Residents’ Report