CBRAC-U REGIONAL TRAUMA SYSTEM PLAN
advertisement

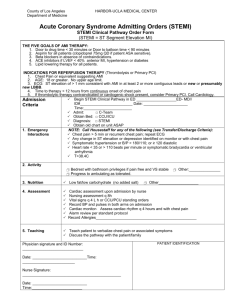
CBRAC-U REGIONAL TRAUMA SYSTEM PLAN BYPASS PROTOCOL FOR THE CONFIRMED ST ELEVATION MYOCARDIAL INFARCTION PATIENT Goal: A ST elevation myocardial infarction (STEMI) which is confirmed with a 12 lead electrocardiogram will be quickly identified and transported to the appropriate percutaneous coronary intervention (PCI) capable chest pain accredited hospital in an expeditious manner. Decision Criteria: This bypass protocol is intended to ensure that patients with a confirmed STEMI will be transported directly to the appropriate chest pain accredited PCI capable hospital. Exceptions to the bypass protocol requiring the patient be transported to the NEAREST facility are: Inability to establish and/or maintain an airway or in the event of cardiac arrest, the patient will be transported to the nearest acute care facility. Transport time to the indicated PCI facility exceeds 30 minutes and EMS is unable to handoff the patient to a higher level of prehospital care, the patient will be transported to the nearest facility. Consideration to bypass the closest facility based on exclusionary criteria for thrombolytics will necessitate contact with that facility or medical director for medical direction. Patient Criteria for Activation of Bypass Protocol for the Confirmed STEMI Patient The activation of the Bypass Protocol for the confirmed symptomatic STEMI patient will be initiated upon the recognition of a confirmed STEMI with 12 lead EKG. Air Ambulance/Hand-Off Hand off of the STEMI patient to advanced life support (ALS)/mobile intensive care unit (MICU)/air transport will be initiated in the following circumstances: If the responding unit is the first/only responder and is unable to leave the service area. Consider air handoff if transport time is greater than thirty minutes. Notes: If there should be any questions regarding activation of treatment protocol for the confirmed STEMI patient, the receiving facility should be contacted for decisions regarding treatment. The receiving facility should be notified at the earliest possible time by EMS to provide the facility with the ability to activate a cardiac team response. Patient’s rights, choices and best interest will be respected in the determination of hospital destination. Thrombolytic Screening Exclusionary Criteria Active internal bleeding History of CVA Recent intracranial or intraspinal surgery or trauma (2 months) Intracranial neoplasm, AVM, or aneurysm Known bleeding diathesis Uncontrolled hypertension (systolic > 185 mmHg and or diastolic > 110 mmHg)