EECP - Anthem
advertisement

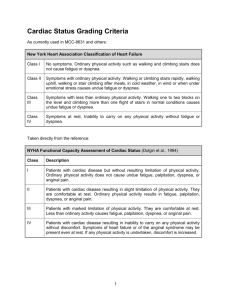
REVIEW REQUEST FOR Enhanced External Counterpulsation (EECP) in the Outpatient Setting Provider Data Collection Tool Based on Coverage Guideline MED.00010 Policy Last Review Date: 05/13/2010 Policy Effective Date: 07/07/2010 Provider Tool Effective Date: 09/29/2010 Individual’s Name: Date of Birth: Insurance Identification Number: Individual’s Phone Number: Ordering Provider Name & Specialty: Provider ID Number: Office Address: Office Phone Number: Office Fax Number: Rendering Provider Name & Specialty: Provider ID Number: Office Address: Office Phone Number: Office Fax Number: Facility Name: Facility ID Number: Facility Address: Date/Date Range of Service: Place of Service: Service Requested (CPT if known): Outpatient Home Inpatient Other: Diagnosis (ICD-9) if known): **Please complete this section before proceeding to request section: Please check all that apply to individual: Cardiac catheterization within 2 weeks (may cause bleeding at the femoral puncture site) Arrhythmias such as Atrial fibrillation, atrial flutter, ventricular tachycardia, and frequent premature ventricular beats (might interfere with the device's triggering mechanism) Aortic insufficiency (regurgitation might prevent diastolic augmentation) Peripheral vascular disease and/or phlebitis (increased risk of thromboembolus) Deep vein thrombosis, varicosities and stasis ulcers Severe hypertension, greater than 180/110 mmHg, (treatment could produce diastolic blood pressure above acceptable limits) Bleeding diatheses Receiving Coumadin (warfarin) therapy with prothrombin time (PT) greater than 15 seconds and/or international normalized ratio (INR) greater than 2.0 (cuffs could cause bleeding in legs) Pregant woman or woman of childbearing potential who does not employ a reliable contraceptive method (possible danger to fetus) Congestive heart failure (CHF) Initial Course Request for the initial single course of enhanced external counterpulsation (EECP) for individual with disabling, chronic, stable angina (if checked, please classify according to New York Heart Association (NYHA) guidelines) CLASS I – Individual with cardiac disease but without resulting limitation of physical activity; ordinary physical activity does not cause undue fatigue, palpitation , dyspnea, or anginal pain; symptoms only occur on severe exertion Page 1 of 2 REVIEW REQUEST FOR Enhanced External Counterpulsation (EECP) in the Outpatient Setting Provider Data Collection Tool Based on Coverage Guideline MED.00010 Policy Last Review Date: 05/13/2010 Policy Effective Date: 07/07/2010 Provider Tool Effective Date: 09/29/2010 CLASS II – Individual has cardiac disease resulting in slight limitation of physical activity; they are comfortable at rest; ordinary physical activity (e.g., moderate physical exertion, such as carrying shopping bags up several flights of stairs) result in fatigue, palpitation, dyspnea, or anginal pain. CLASS III – Individual has cardiac disease resulting in marked limitation of physical activity; they are comfortable at rest; less than ordinary activity causes fatigue, palpitation, dyspnea or anginal pain. CLASS IV – Individual has cardiac disease resulting in the inability to carry on any physical activity without discomfort; symptoms of heart failure or the anginal syndrome may be present even at rest; if any physical activity is undertaken, discomfort is increased. Treatment for a total of 35-36 hours of EECP; administered for one to two hours daily, 5 days a week, for approximately 3½ to 7 weeks Individual is refractive to optimal medical therapy Individual is not readily amenable to surgical intervention such as percutaneous transluminal coronary angioplasty (PTCA) or cardiac bypass due to: (check any that apply) Individual’s condition is inoperable Individual is at high risk for operative complications or postoperative failure Individual’s coronary anatomy is not readily amenable to such procedures Individual has comorbid states which create excessive risk Other (please list) Other (please list) Repeat Course Request for repeat course of therapy for individual with chronic stable angina who has objectively demonstrated response to EECP (check any that apply): Individual demonstrates early improvement in radionuclide stress perfusion imaging compared to a pre-EECP baseline Individual demonstrates reduction in antianginal medication use Individual demonstrates improvement in exercise tolerance Other (please list) Others (please list) This request is being submitted: Pre-Claim Post–Claim. If checked, please attach the claim or indicate the claim number I attest the information provided is true and accurate to the best of my knowledge. I understand that Anthem may perform a routine audit and request the medical documentation to verify the accuracy of the information reported on this form. _____________________________________________________________ Name and Title of Provider or Provider Representative Completing Form and Attestation (Please Print)* Date *The attestation fields must be completed by a provider or provider representative in order for the tool to be accepted Anthem UM Services, Inc., a separate company, is the licensed utilization review agent that performs utilization management services on behalf of your health benefit plan or the administrator of your health benefit plan. Page 2 of 2