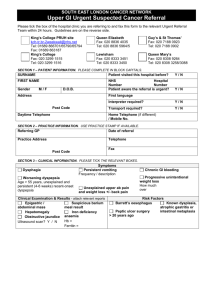
Upper GI Checklist and Referral Form

Upper GI Checklist and Referral From
Contact details:
Referral Date
Address
GSTT
Phone
~[Today...]
KCH
Patient Name ~[Forename]
~[Surname]
DOB ~[Date Of Birth]
Other
Referring
Clinician
Practice
Details
~[Free Text:Referring
Clinician?]
~[Surgery Address
Line 1]
~[Surgery Address
Line 2]
~[Surgery Address
Line 3]
~[Surgery Address
Line 4]
~[Surgery Tel No.]
Patient
Address
~[Patient Address
Block]
Patient Tel
Mobile
~[Telephone Number]
~[Mobile]~[Mobile
Number]
NHS Number ~[NHS Number]
Hospital ~[Hospital Number]
Number
Referral Checklist
1. Have you considered the 2 week wait criteria
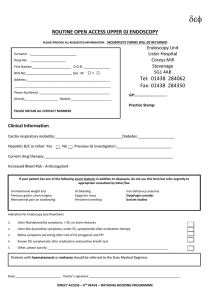
2. Are you referring for Direct Access Endoscopy?
Yes
Yes
No
No
3a) Have you reviewed the patient’s medication use (e.g. NSAIDs/ Aspirin/ Prednisolone/ Prokinetics) as well as over the counter medications?
Yes No
3b) What medications have been tried (e.g. PPI for 4 weeks, H2 antagonist, alginate)
Please list medication: Duration:
4. Have you tested for Helicobacter pylori? Positive Negative
If positive was first line treatment given? Yes No
5. If you have answered no to any of the above, please list reason for referral (including any other relevant information):
Final Version - March 2013
Medical history & examination
History of presenting symptoms:
Past Medical History: ( Diabetes/ IHD/ Hypertension)
Anaemia Results Hb: MCHC Ferritin
Drugs History + Allergies
Smoking status ~[ReadCode:TREF:8022~1Y~~R~Date|Free Text~0] If yes cigarettes/ day
Alcohol use (units per week) ~[ReadCode:136~1Y~~R~Date|Free Text~1]
Weight / BMI ~[ReadCode:22A~1Y~~R~Date|Free Text~1]/~[ReadCode:22K~1Y~~R~Date|Free
Text~1]
Information
NOTES :
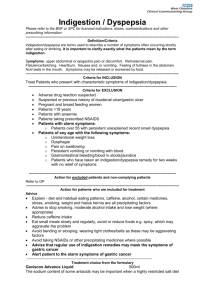
Two week wait criteria – refer urgently any patients presenting with:
Dysphagia
Unexplained upper abdominal pain and weight loss, with or without back pain
Upper abdominal mass with or without dyspepsia
Obstructive jaundice (depending on clinical state)
Patients of any age with dyspepsia and any of the following o Chronic gastrointestinal bleeding o Progressive unintentional weight loss o Persistent vomiting o Iron deficiency anaemia o Epigastric mass o Suspicious barium meal result
Patients aged 55 years and older with unexplained and persistent recent-onset dyspepsia alone.
Consider an urgent referral for patients presenting with:
Persistent vomiting and weight loss in the absence of dyspepsia
Unexplained weight loss or iron deficiency anaemia in the absence of dyspepsia
Unexplained worsening of dyspepsia and o Barrett’s oesophagus o Known dysplasia, atrophic gastritis or intestinal metaplasia o Peptic ulcer surgery over 20 years ago.
Direct Access Endoscopy
Please ensure patients are withdrawn from PPI two weeks prior to endoscopy
Minor GI bleed (no evidence of active bleeding)
Abnormal Barium swallow/ Meal
Symptoms which persists following a trial of H2 receptor antagonist & H.pylori negative
H pylori
If first line treatment failed has second line treatment been given
Quadruple therapy for 2 weeks with tripotassium dicitratobismuthate , tetracycline, metronidazole and a proton pump inhibitor is recommended in case of treatment failure
Routine testing to confirm eradication is not necessary , unless the patient has H.pylori associated peptic ulcer