Lung v5 - Frimley Park Hospital
advertisement

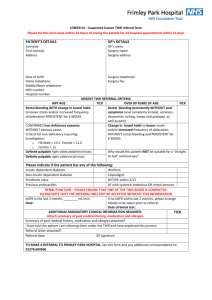
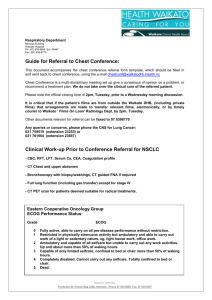
LUNG – Suspected Cancer TWR referral form Please fax this form back within 24 hours of seeing the patient for 24 hospital appointment within 14 days PATIENT’S DETAILS GP’s DETAILS Surname First name(s) Address GP’s name Surgery name Surgery address Date of birth Surgery telephone: Home telephone: Surgery fax: Mobile/Work telephone: NHS number: Hospital number: Patients with STRIDOR or SIGNS of SUPERIOR VENA CAVAL OBSTRUCTION (i.e. swollen face/neck with fixed jugulat venous pressure elevation) ADMIT IMMEDIATELY URGENT TWR REFERRAL CRITERIA TICK Persistent haemoptysis in smokers or ex-smokers aged 40 or older A chest X-ray suggestive of lung cancer including pleural effusion and slowly resolving consolidation A normal x-ray where there is a high suspicion of lung cancer A history or asbestos exposure with recent onset chest pain/breathlessness/unexplained systemic symptoms, where a chest x-ray indicates pleural effusion, pleural mass or any suspicious lung pathology RENAL FUNCTION – PLEASE ENSURE THAT ONE OF THE TWO BOXES IS COMPLETED PLEASE NOTE THAT THE REFERRAL WILL NOT BE ACCEPTED WITHOUT THIS INFORMATION eGFR in the last 2 months ________ mL/min If no eGFR within last 2 months, please arrange Date: bloods to be taken prior to referral. Date of blood test: PATIENTS WHO NEED AN URGENT X-RAY (REPORTED WITHIN 5 DAYS) INCLUDE: Unexplained or persistent (longer than 3 weeks) Haemoptysis Chest and/or shoulder pain Neck or supraclavicular lymph nodes Dyspnoea Underlying chronic Cough Weight loss respiratory problems with Features suggestive unexplained changes in Chest signs metastasis from lung cancer existing symptoms Hoarseness (brain/bone/liver/skin etc) Finger clubbing ADDITIONAL MANDATORY CLINICAL INFORMATION REQUIRED: Attach summary of past medical history, medication and allergies Summary of past medical history, medication and allergies attached? I have told this patient I am referring them under the TWR and have explained this process Referral letter attached? Referral date: GP signature TICK TO MAKE A REFERRAL TO FRIMLEY PARK HOSPITAL, fax this form and any additional correspondence to: 01276 604506