Referral to LivingCare
advertisement

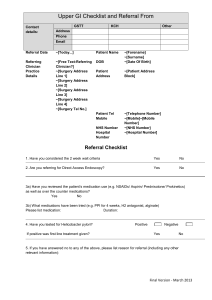
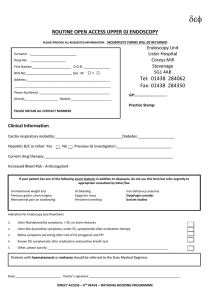
Upper GI Endoscopy referral form Priority: urgent routine We will contact your patient by telephone to offer an appointment. Please ensure we have a contact number, preferably a mobile number, so that treatment is not delayed. Mr/Mrs/Miss Surname First name(s) NHS number Gender Address Referral criteria 55 or over with unexplained and persistent RECENT onset dyspepsia Dyspepsia, or upper GI symptoms, at any age if associated with a strong family history of significant upper GI disease Upper GI symptoms which have not responded to symptomatic trial of dyspepsia management. This should include HP testing Unexplained worsening of dyspepsia with one of the following risk factors – Barretts/ pernicious anaemia/previous peptic ulcer surgery Asymptomatic, iron deficiency anaemia in men and postmenopausal women HB MCV Ferritin Patients with positive coeliac antibodies, requiring confirmatory upper GI endoscopy and biopsy Recent hospital admission requesting GP to arrange upper GI endoscopy Progressive dysphagia Persistent vomiting Patients requiring Barrett’s surveillance Signature of GP: Date: Date of birth Referring GP Registered GP Practice code Practice address Yes No HP eradication Yes Current treatment PPI Aspirin NSAIDS Warfarin Other significant medication Allergies Patients with the following are not suitable for open access endoscopy and should be referred to a gastroenterology clinic: Where endoscopy will not alter management Myocardial infarction within the past eight weeks Moderate or severe cardiac or respiratory disease Elderly/frail patients Patients who are receiving chemotherapy Immunosuppressed patients Patients who cannot give informed consent to the procedure No