Physical Examination of the
newborn infant
新生兒檢查
高醫小兒科部 新生兒科
作完整新生兒檢查之準備事項
• 作完整新生兒檢查之時機︰在餵食之後約1到2個
小時,因為此時嬰兒比較不會想睡或太飢餓。
• 維持溫暖的環境來作檢查。若可以的話,可使用
頭頂的輻散發熱器 (radiant warmer)。
• 除尿布之外,除去外部衣服,以作全身之檢查
• 在檢查期間,你需要使用溫和、輕柔的聲音;並
對嬰兒微笑。
• 儘量使檢查流程順利,不要突然嚇到嬰兒。
• 作較侵犯性的檢查時,可使用安撫奶嘴。
新生兒檢查之順序
在嬰兒生命徵象穩定之後,按照以下之檢查順序,進行新生兒檢查。
1. 除去外部衣服,留下尿布。
2. 測量頭圍、身長及體重並將其畫在生長曲線圖上。
3. 摸前囟門(anterior fontanelle),感受其張力(tension)是否正常或是有凹
陷之情形。並檢查頭顱。
4. 注視嬰兒的臉,看其膚色及是否有異常之處。
5. 檢查眼睛,耳朵,鼻子和嘴。
6. 檢查頸部,包括觸摸鎖骨。
7. 聽心音及呼吸音,並估計心跳速率和呼吸速率。
8. 摸腹部。
9. 檢查手臂、手、腿和腳。
10. 打開尿布,並摸其股動脈脈搏。
11. 檢查生殖器、肛門口及臀部。
12. 把嬰兒轉向俯臥的位置並且檢查背部和脊椎,並評估肌肉張力。
13. 將嬰兒轉回仰臥位置,評估中樞神經系統(CNS)。
14. 確保你沒忽略任何事情,並且你也已經檢查母親所注意的任何現象
Measurements
• Measure body weight
• Check Body length
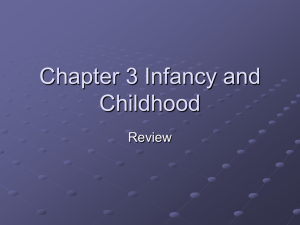
• Check head circumference
– The tape should encircle the
most prominent parts of the
forehead and occiput
From Pediatric clinical skills P.27
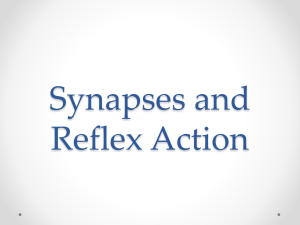
Skin color
• Reddish pink – healthy warm babies
• Generalized redness of the skin, plethora -- ploycythemia
• White cheesy vernix
• Dry, cracked, or peeling skin – post-maturity
• Greenish – meconium
• Bruising and petechiae – birth process or need further
evaluation
• Pallor – anemia or peripheral shutdown with shock or both
• Jaundice – normally, it appears between 2 and 4 days
• Mottled skin – cutis marmorata
Jaundice
Mottled skin
Normal skin color
Pallor and malnutrition
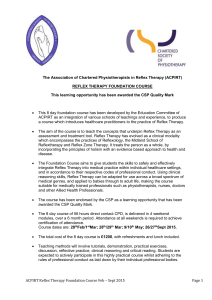
Skin rashes
• Milia
• Erythema toxicum
• Transient neonatal
pustular melanosis
• Acne neonatorum
• Herpes simplex
• Macular hemangioma
(stork bites)
• Port-wine stain (nevus
flammeus)
• Mongolian spot
• Cavernous hemangioma
• Strawberry hemangioma
(macular hemagnioma)
Erythema toxicum
Acne neonatorum
Seborrhic dermatitis
Milia
Mongolian spot
Mongolian spot
Macular hemangioma
Strawberry hemangioma
Port-wine stain
Erythema
toxicum
Epidermal nevi
syndrome
Leukemia cutis—
multiple brown-red to violaceous papules and nodules
From assessment and care of the well newborn 2nd edition, color plate 12
Head and skull
•
•
•
•
•
Distorted and molded – normal
Size -- normally in 32-38 cm at term
Anterior fontanel -- for tension and size
Cranial sutures -- up to 1 cm is normal
Caput succedaneum -- edema caused by
pressure over the presenting part; crosses
suture lines
• Cephalohematoma -- collections of blood
between the periosteum and the skull
bones; most in the parietal; do not extend
across the suture lines
• Subgaleal hemorrhage – fluctuant; blood
accumulation beneath the scalp in a large
space
microcephaly
Cephalohematoma
From Pediatrics 2005, Mosby, Inc. p17 &1262
Ear and nose
• low-set ears
• Note any pre-auricular
pits, skin tags or
accessory auricles
• Nose: general shape and
width of the bridge
Normal ear position
From Pediatrics 2005, Mosby, Inc. p18
microtia
Eyes
• Note gross abnormality, size, dimensions and slant,
persistent
• Strabismus or nystagmus
• Ophthalmoscopic examination: not practicable
• Slight mucoid discharge: sticky eye; very common
in the first 2 days later
• Subconjunctival
hemorrhages:
very common after birth,
harmless
• Hypertelorism
• Hypoterlorism
From Physical diagnosis in neonalology P.249
Cornea
• Normal: bright and clear; size 10mm
• If cornea size is greater than 13mm
(particularyly if the cornea is also hazy):
congenital glaucoma
• Cataracts: can be occasionally seen with the
naked eye using a bright light shone
tangentially
From: www.hksh.com
From: bayshoreophthalmology.com/servicesglaucoma.htm
from: www.snec.com.sg/clinical/glaucoma.asp
Mouth
• Note micrognathia;
• any asymmetry of the corners of
the mouth and the nasolabial
folds
– Facial nerve palsy
– An absent angularis oris muscle
• Palate: intact or cleft or higharched or grooved
• Minor variations:
From Atlas of Neonatology 7th edition
– Epstein's pearls,
– Natal teeth,
– Short frenulum or tongue tie
From Atlas of Pediatric Physical Diagnosis 3rd edition p40 &
Physical diagnosis in neonalology P.216
Pierre-Robin sequence –
the association of an often wide U-shaped cleft palate with a
small mandible and a posteriorly placed tongue
Neck
• Webbed neck: Turner syndrome
• Redundant skin posterior: one of the
characteristics of Down syndrome
• Cystic hygromas: soft fluctuant swellings; most
arising in the posterior triangle
• Sternomastoid tumors: hematoma in the
sternomastoid muscle
• Clavicle: should be palpated for fractures => Erb's
palsy or shoulder dystocia
Chest
• Breast swelling + a few drops of 'witches'
milk: quite normal
• Respiratory rate: normally 40-60
breaths/minute
• Respiratory pattern: flaring of the alae nasi,
grunting, retractions
• Auscultation: bowel sounds in the chest =>
asymptomatic diaphragmatic hernia
Cardiorespiratory system
• Palpate the precordium: thrills or pronounced ventricular
heave
• Point of maximal impulse: usually found in the L't 4th
intercostal space inside the mid-clavicular line
• Check the peripheral pulses: if PDA + significant L't to R't
shunt bounding pulse
• Heart rate: abnormally fast (>160/min) or slow (<100/min)
• Check if there is heart murmur
• Signs of heart failure: tachycardia, tachypnea,
hepatomegaly
• Measure the blood pressure: not practicable
Abdomen
• Abdominal distension: easily appreciated
• Umbilicus:
–
–
–
–
–
–
Three vessels
any discharge or reddening of the skin
Thick cord with profuse jelly => diabetic mother
Thin one => small-for-dates babies
Green discoloration: meconium stain => intrauterine asphyxia
Note umbilical hernia
• Palpate the abdomen: liver edge -- can be up to 2 cm
below RCM
• Kidneys -- detect any abnormal large renal mass
• Spleen -- just tipped; if > 1 cm => investigation
• Auscultation: suspect GI problem ex. distension, bilestained vomiting, failure to pass meconium, or bloody
stools
Genitalia-Male
• Penis:
– Normally about 3 cm; phimosis is usual
• Check the position of urethral meatus
– Hypospadias as glandular, coronal,
mid-shaft or perineal
• Inspect the shaft of the penis
• Check the urinary stream: meatal stenosis
with hypospadias; urethral valve
• Scrotum:
– Testes -- both should be palpable in full term
– Hydroceles -- resolve spontaneously
• Note inguinal hernia
Hydrocele
Inguinal hernia
Hypospadias
From Pediatrics 2005, Mosby, Inc. p1353-1354
Bifida scrotum with hypospadias
Genitalia- Female
• Vulva: the clitoris and labia minora
are relatively prominent
• White mucoid vaginal discharge
with blood stained – normal
• Small skin tags or mucoid cysts -can resolve spontaneously
Anus
• Check the position of
the anus and anal tone
• By spreading the
buttocks apart as a
superficial dimple may
resemble an anus
Imperforated anus with
fistula
Ambiguous genitalia
From Pediatrics 2005, Mosby, Inc. p1359
Upper limbs
• Inspect the arm: shape,
posture, symmetry
• Examine the hand: flexion
deformities of the fingers;
palm creases; syndactyly or
polydactyly
• Observe spontaneous arm
movements
• Erb’s palsy -- lack of
movement in the arm and the
hand showed 'waiter's tip'
position
From Atlas of Neonatology 7th edition
Clenched hand
Lower limbs
• Inspect the legs and feet: posture, symmmetry, general size
and shape
• Observe spontaneous or stimulated active movements:
restriction of joint
• Feet: 'Rocker bottom' shape and short hallux => Edward
syndrome
• Puffy feet and hypoplastic nails => Turner syndrome
• Calcaneovalgus position => fetal position in utero
• Equinovarus position
• Over-riding toes: self-correcting
Trisomy 18
Edward syndrome
Hip
• Congenital dislocation:
common following breech
presentation; most of girls
• Perform Ortolani's test &
Barlow's test
From Physical diagnosis
in neonalology P.417
Neurological examination
• Formal testing is seldom needed
• Posture: normal neonate -- lies predominantly in a
flexed position
• The presentation at birth can influence posture for
several days
• Spontaneous motor activity
• Muscle tone and strength: test by
– Assessing resistance to passive movements
– Pull-to-sit maneuver
– Ventral suspension
• Crying: note if it is either-high pitched or very weak
• Feeding and sucking patterns
• Reflex responses: Moro reflex, Grasp reflex, Rooting
and sucking reflex
Primitive reflexes
Rooting reflex
Sucking reflex
Grasp reflex
Grasp reflex
Moro reflex
Thanks for your attention !