Essential Elements of the
Neuro Exam
Your Guide:
JJ Baumann, MS, RN,CNS
The brain is the last and grandest
biological frontier, the most
complex thing we have yet
discovered in our universe.
It contains hundreds of billions of
cells interlinked through trillions of
connections.
The brain boggles the mind.
~ James D. Watson
(from Discovering the Brain, National Academy Press,
1992)
Why know what’s inside?
• Direct what to look for
in the neuro exam
• Impact be on the
patient’s life
• Location of lesion
• Type of lesion
– Anatomical: trauma
– Physiologic: metabolic,
infectious
– Conductive: epileptic
The Hard Candy Shell
Meninges
• Collective term
for covering of
brain
• Attached brain to
bony structures
• Supports
• Protects
• Encloses
Name this tumor!
• Dura Mater – covers all of brain
• Arachnoid Mater – thin, clear, avascular, houses
CSF
• Pia Mater – gives brain shape, forms sulci and
gyri
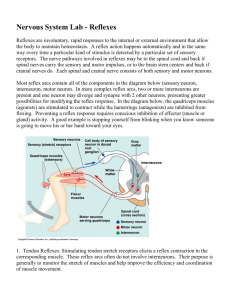
Name that bleed!
Usually caused by a
blow to the temporal
area
Caused by tearing of
arteries (esp medial
meningial)
Bleeds fast
Pt has labile alertness
Above the dura
Name this bleed!
Can by sudden or
gradual
Caused from the
break in bridging
veins
Seen in very young
and very old
Bleed is under the
dura
Name that bleed!
Usually occurs while
straining on the toilet
or post coital
75% caused from a
cerebral aneurysm
Pt complains of the
worst HA of their
entire life
Bleed is below the
arachnoid space
The Soft Center
Frontal Lobe
•
•
•
•
•
•
Extends all the way to the central sulcus
Judgment, personality, and reasoning
Initiates motor function
Bowel and bladder
Broca’s speech
Long term memory (phone #s)
Summary – this lobe makes you acceptable to be
in public.
Temporal Lobe
•
•
•
•
•
Lobe sits in sphenoid bone
Wernickes speech area
1º hearing - listening to voice
2º hearing - interpretation of voice
Short term memory
Summary: Husbands have temporal lobe
damage.
Parietal Lobe
• Posterior central sulcus
• Processes tactile stimulation to modulate
movement
• Stereognosis (recognize object by feeling
size and shape)
• Two point discrimination
Summary: Robots do not have parietal
lobes!
Occipital Lobe
• 1º vision – see object
• 2º vision – interpret / relate to previous
experience
Summary: Mom does see out the back of
her head!
Cerebellum
Helps provide smooth, coordinated body
movements.
• Tremors.
• Nystagmus (Involuntary movement of the
eye).
• Ataxia, lack of coordination.
Brain Stem
• Midbrain – CN 3 & 4
• Pons – Pontine pupils, respiratory drive
CN 5 - 8
• Medulla - Crossing of motor tracts.
Cardiac and Vasomotor Center
Respiratory Center
CN 9-12
Alzheimer’s
Progressive memory loss.
Declining interest in people and
environment.
Episodic bouts of irritability.
Neglects personal hygiene.
What lobes are effected?
Michael J. Fox, actor (quoted in
People magazine, December 7, 1998,
p. 135; talking about his surgery for
Parkinson's disease)
They did something once that
slurred my speech, and I thought,
"Oh, man, you're messing with my
brain. It's freaking me out."
What part of the brain did
they mess with?
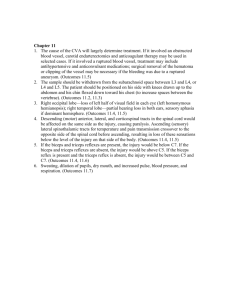
Infratentorial
Infratentorial: Infratentorial Hernations. From Betz et al., 1994.
No Fat, Just Brain
ICA – Big Time
• Contralaterial sensory and motor
• Aphasia – if dominant hemisphere
involved
• Agnosia, unilateral neglect – if non
dominant hemisphere is involved
• Contralateral visual field deficit / eye
deviation
ACA – Crazy Legs
•
•
•
•
•
•
Paralysis of contralateral foot and leg
Sensory loss –toes, foot, leg
Impaired gait
Abulia (slow to respond)
Flat affect
Urinary incontinence
MCA – The Drift
• Motor and sensory of face and arm on
contralateral side
• Global aphasia if dominant hemisphere
involved
• Neglect if non-dominant hemisphere
involved
• Homonymous hemianopsia
PCA / Pcom
• Contralateral visual field deficit, impaired
depth perception, nystagmus, sensory loss
• Ipsilateral 3rd nerve palsy
Big Bad Basilar
• Quadriplegia
• ‘locked-in’
• Weakness of facial, lingual, and
pharyngeal muscles
Name that vessel.
Pt presents with:
• L facial droop
• L sided arm
weakness
• Aphasic
Drainage
Frontal and parietal
veins drain to superior
sagittal sinus.
Inferomedial veins drain
to straight sinus.
Then drain to large
venous sinus and to
jugular veins.
Traveling with CSF
Choroid plexus and
ependymal cells –
lateral ventricles –
foramen of Monroe –
3rd – aqueduct of
sylvius – 4th then
absorbed by
arachnoid villi meets
with sag sinus and
into venous
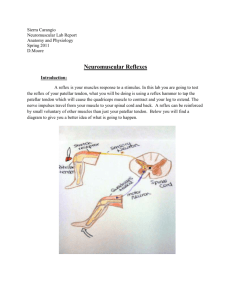
Monro-Kellie
Doctrine
Increasing ICP
•
•
•
•
Headache
Nausea
ALOC, lethargy
Cushing’s Triad
– Widening pulse
pressure
– Bradycardia
– Irregular respirations
EVD
•
•
•
•
Drain blood and CSF
Monitor ICP (<20)
Monitor CPP (70-90)
HOB >30
What in the brain is going on here?
•
•
•
•
Ischemic?
Hemorrhagic?
Seizure?
Other neuro
problems?
• Onset?
• Changes in neuro
status?
• Level of
consciousness?
• Numbness /
tingling?
• Focal weakness?
• Coordination?
• Trouble speaking or
understanding
others?
The Neuro Physical Exam
•
•
•
•
•
•
Mental status
Cranial nerves
Motor system
Sensory system
Coordination
Deep tendon
reflexes
Glasgow Coma Scale
Intro – Survey the Scene
Full consciousness
Confusion
Lethargy
Obtunded
Stupor
Coma
Can we talk?
• Oriented to person, place, time, and
event?
• Rate, rhythm , and articulation of speech?
• Expressive or receptive aphasia?
• Intact memory? (Remember three simple
words)
Facing Cranial Nerve
Assessment, Barbara
Bolek, American
Nurse Today,
November 2006
Cranial Nerve Function
CN I Olfactory
Close eyes, close one nostril at
a time, smell, identify
CN II Optic
Read newspaper
Close one eye, move finger,
"tell me when you see it"
Copyright Nursing Brains, LLC
Cranial Nerve - Midbrain
CN III Oculomotor Pupil size, shape, react to light
Assess eye lid (ptosis)
CN IV Trochlear
CN VI Abducens
Move finger in "H"
Copyright Nursing Brains, LLC
Cranial Nerves - Pons
CN V Trigeminal
Separate clenched jaw
Corneal reflex
Assess touch of forehead, cheek, chin
CN VII Facial
Show teeth, puff out cheeks
Identify sugar on tongue
CN VIII Acoustic
Rub strands of hair together
Whisper at foot of bed
Copyright Nursing Brains, LLC
Cranial Nerves - Medulla
CN IX Glossopharyngeal Say "AAH", check symmetrical
CN X Vagus
elevation of uvula
Check gag, both sides of uvula
CN XI Spinal Accessory Push head against hand, both sides
Shrug shoulders against resistance
CN XII Hypoglossal
"Stick out your tongue", check
midline placement
Copyright Nursing Brains, LLC
Motor Function
• Assess for muscle size and tone
bilaterally.
– Spasticity (Upper motor neuron injury)
– Rigidity
– Flaccidity (Lower motor neuron injury)
• Assess gait and posture
• Look for involuntary movements.
• Assess muscle strength.
Muscle Strength Grading
0 = No movement
1 = Trace of muscle contraction
2 = Active movement without
gravity
3 = Active movement against
gravity
4 = Active movement against
gravity / resistance
5 = Normal
NIH SS
0 = No drift; limb holds 90 (or 45)
degrees for full 10 / 5 seconds.
1 = Drift; limb holds 90 (or 45)
degrees, but drifts down before
full 10 / 5 seconds; does not hit
bed or other support.
2 = Some effort against gravity;
limb cannot get to or maintain (if
cued) 90 (or 45) degrees, drifts
down to bed, but has some effort
against gravity.
3 = No effort against gravity; limb
falls.
4 = No movement.
Lyden P, BrottT,Tilley B, et al; Group NTSS.
Improved reliability of the NIH stroke scale
using video training. Stroke. 1994;25:22202226.
Sensory Function
• Assess touch – soft and sharp – in each of
the dermatomes.
• Assess temperature and vibration
bilaterally.
• Proprioception – thumb or big toe are
moved up and down. Patient able to state
correct location without looking.
Discriminative Sensation
• Two-point discrimination – part of body is
touched with two sharp objects
simultaneously and asked if can feel one
or two picks.
• Stereognosis – ability to identify a familiar
object in hand (no peeking!)
• Graphesthesia – draw # or letter in
patients hand and have them correctly
identify it.
Coordination
DTRs
Biceps – C5
• The biceps reflex is
elicited by placing
your thumb on the
biceps tendon and
striking your thumb
with the reflex
hammer and
observing the arm
movement.
Brachioradialis – C6
• The brachioradialis
reflex is observed by
striking the
brachioradialis tendon
directly with the
hammer when the
patient's arm is resting.
Strike the tendon
roughly 3 inches above
the wrist. Note the
reflex supination.
Repeat and compare to
the other arm.
Triceps – C7, 8
• The triceps reflex is
measured by
striking the triceps
tendon directly with
the hammer while
holding the patient's
arm with your other
hand.
Patellar – L3,4
• With the lower leg
hanging freely off
the edge of the
bench, the knee jerk
is tested by striking
the quadriceps
tendon directly with
the reflex hammer.
Achilles – S1,2
• The ankle reflex is
elicited by holding
the relaxed foot with
one hand and
striking the Achilles
tendon with the
hammer and noting
plantar flexion.
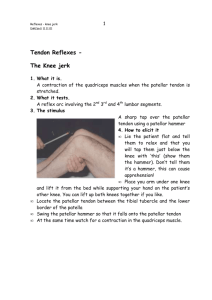
Babinski Reflex
• The plantar reflex
(Babinski) is tested by
coarsely running a key
or the end of the reflex
hammer up the lateral
aspect of the foot from
heel to big toe. The
normal reflex is toe
flexion. If the toes
extend and separate,
this is an abnormal
finding called a positive
Babinski's sign.
Reflexes
• Deep Tendon Reflexes
– Biceps, triceps, brachioradialis, patellar, achilles
• Superficial Reflexes
– Epigastric, abdominal, cremasteric, gluteal, plantal,
bulbocavernous, superficial anal
• Brain Stem Reflexes
– Pupillary reaction, corneal, oculocephalic,
oculovestibular, gag
• Pathological Reflexes
– Babinski, grasp
Copyright Nursing Brains, LLC
DTR Reflex Scale
0 : absent reflex
1+: trace, or seen only with reinforcement
2+: normal
3+: brisk
4+: nonsustained clonus (i.e., repetitive
vibratory movements)
5+: sustained clonus
As we begin the 21st century, the Hubble
space telescope is providing us with
information about as yet uncharted
regions of the universe and the promise
that we may learn something about the
origin of the cosmos. This same spirit of
adventure is also being directed to the
most complex structure that exists in the
universe - the human brain.
Floyd E. Bloom (in Fundamental Neuroscience edited by L.R. Squire et al.,
2003)
Questions?