Readmissions Powerpoint
advertisement

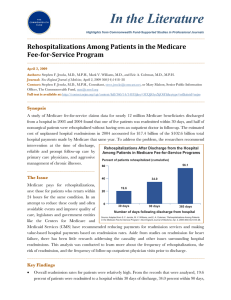
Patients’ Needs Clinical/Financial Stability and Patient/Resident/Client Satisfaction Vibra, ARU, SNFs, HHA, et al Collaboration for Improved Clinical Outcomes Physicians and staff working as partner for patient care Value of monitoring utilization of resources Timely transitions: “Right level of care at the right time” The Affordable Care Act of 2010 requires HHS to establish a readmission reduction program. 20% of Medicare patients are readmitted to a hospital within one month of discharge CMS’ goal to transition to value based purchasing-paying for care based on quality and not just quantity Initial focus- AMI, CHF and pneumonia; 2015 possibilities- MedPAC recommendations of COPD, CABG and PTCA procedures, and other vascular procedures Penalties- Oct 2012- 1%; Oct 2013- 2%; Oct 2014- 3% The Continuum of Healthcare Sites of Service High ACUTE CARE HOSPITALS Intensity of patient service LTACHs Low SKILLED NURSING FACILITIES TRANS CARE OUTPATIENT REHAB TRANS CARE ICU SUBACUTE & INPATIENT REHAB CHRONIC CARE ASSISTED LIVING HOME HEALTH CARE HOSPICE ADULT DAY CARE HOME Low Severity of patient illness High Breakdown of Inpatient Readmission Source 64% Home w/o any post acute care 20% Skilled Nursing Facilities 11% Home w/home health care 5% Rehab , LTACH or Psych Hospitals Source: Health Care Financing Review| 2009 data Current Industry Issues § Highly fragmented market of hospitals and PAC providers § Economic incentive for acute care providers to increase PAC patient volume and rapidly discharge § No coordination of patients over episode of care § No economic penalty for poor performance Medicare Policy is Rearranging the Post-Acute Landscape ____________________ Source: RTI International, 2009, “Examining Post Acute Care…” and Avalere Health, LLC, “Change in the SNF Marketplace” March 2012. Same Source for next slide National Statistics 23% are Readmitted to Hospital 35% of Hospital Discharges are Admitted to PostAcute for Additional Care (“Post-Acute Admissions”) 48% of Post-Acute Admissions go Home after Receiving Post-Acute Care 29% are Transferred to a Secondary Post-Acute Venue for Additional Care Medicare Statistics 30-day Risk Adjusted Readmission Rates for a Portland Hospital Measure Number of Patients Readmission Rate National Average Heart Attack 209 18.0% 19.7% Heart Failure 201 28.0% 24.7% Pneumonia 109 18.7% 18.5% Source: America Hospital Directory, 07/01/2008 to 06/30/2011 posted on 04/12/2013 Long Term Acute Care- MS DRGs Skilled Nursing facilities- RUGs and per diem Foster Home- per diem; Medicare not accepted Home Health- DRGs Hospice- per diem Present- MS DRGs ◦ MCC ◦ CC ◦ Non-CC Future Length of Stay ◦ Short Stay ◦ Long Stay ◦ Medicare median Opportunities 1. Improved clinical outcomes and patient satisfaction through coordination of care. 2. Right level of care at the right time for optimal patient care outcomes. 3. Partnerships for coordination of care Thank You! Coming together is a beginning. Keeping together is progress. Working together is success. - Henry Ford



![[Lodi Memorial] Readmission Evaluation Tool](http://s3.studylib.net/store/data/005897421_1-bed185955272958f26cfef7b1d7de2a8-300x300.png)