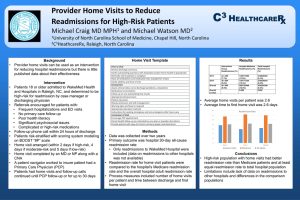
Seven Home-Health Touch
Points to Prevent Avoidable
Re-hospitalizations
Jennifer Wieckowski, MSG
Program Director, Care Transitions
Health Services Advisory Group of California, Inc.
(HSAG of California)
1
Statewide Readmission Reports
Medicare Fee-For-Service (FFS) Data
CY 2012 All-Cause 30-Day Readmission Rates
Setting Discharged To
Number of
30-Day
Number of
Discharges
Readmit
Discharges Readmitted
Rate
Within 30 Days
% of 30-Day
Readmits to
Another
Hospital
Home
383,017
66,102
17.3%
26.6%
Skilled Nursing Facility
173,919
38,317
22.0%
27.2%
Home Health Agency
124,008
25,045
20.2%
22.0%
Hospice
Other
All
15,968
53,449
750,361
553
10,822
140,839
3.5%
20.2%
18.8%
36.9%
41.6%
27.1%
2
Statewide Readmission Reports
Medicare FFS Data (cont’d)
CY 2012 Number of Days from
Discharge to Readmission
Number of
Setting Discharged To
Readmissions
66,102
Home
38,317
Skilled Nursing Facility
25,045
Home Health Agency
553
Hospice
10,822
Other
140,839
All
1–7
Days
36.0%
32.5%
36.3%
44.5%
38.2%
35.3%
8–14
Days
24.9%
25.9%
26.1%
26.2%
22.0%
25.2%
15–21
Days
19.5%
20.9%
19.0%
15.4%
18.5%
19.7%
22–30
Days
19.6%
20.7%
18.5%
13.9%
21.4%
19.8%
3
The Team
Cedars-Sinai Medical Center (CSMC)
Largest private, not-for-profit medical center in
the western United States, with 923 beds
Consistently named one of America’s Best
Hospitals by U.S. News & World Report
Accredited Home Health Services
Ranked in top 2 percent in the country
In business over 33 years
Five locations throughout
Southern California
Monthly census of more than
700 patients
4
The Challenge
Reduce readmissions
from home health by
50 percent.
5
6
Enhanced Home Health Program
Enhanced Home Health Program
Minimum
of
seven
touch
points within two weeks of discharge
A minimum of 7 touch points to occur within the first two weeks of discharge.
Week 1
Week 2
Pre-Discharge
Introduction
Hospital Visit or
Phone Call
Three to Four
Home Visits
Including a Visit
within 24–48
Hours
Tuck-in Phone
Call the 1st
Friday
the Patient is at
Home
Home Visit the
First Weekend
the Patient is
Home
Two to Three
Home Visits
Tuck-in Phone
Call the 2nd
Friday
the Patient is at
Home
Home Visit the
2nd Weekend
the Patient is at
Home
Additional
Home
Health Visits
as Needed
7
Results
Patient Population
Time Frame
Percent
Readmitted
(All-Cause)
Cedars-Sinai discharges
home with home health
(any agency)
July 2010–June 2011
19%
Cedars-Sinai discharges
home with Test of Change
home health agency*
July 2010–June 2011
14%
Test of Change
(n=59 patients)
November 2011
6.8%
* The agency selected for the test of change had the highest proportion of home-health referrals from
Cedars-Sinai Medical Center .
8
8
Adaptability and Spread
Four high-volume home health agencies tested the Enhanced Home
Health program during a six-week period in February and March
2012. A total of 396 patients were enrolled.
Home
Health
Agency
BASELINE
Percentage 30-day
Readmissions
Feb. 2011–Jan. 2012
TEST OF CHANGE
Percentage 30-day
Readmissions
Feb. 15–Mar. 31, 2012
NUMBER OF
PATIENTS
enrolled in TOC
Feb. 15–Mar. 31, 2012
Accredited
12.7%
10.3%
121
Agency II
12.1%
7.8%
103
Agency III
14.7%
11.8%
110
Agency IV
17.3%
6.4%
62
35%
Reduction
9
9
Lessons Learned
Increase in personnel time dedicated to the
program
Communication—frequent and clear
In-patient phone call vs. visit
Patient refusal
10
What You Can Do By Tuesday
Know your readmission rates.
− medicare.gov
Know where your referrals are going.
Develop partnerships.
Improve communication.
Implement tuck-in phone calls.
11
California Rate of Readmissions
Within 30 Days per 1,000 Beneficiaries
Readmissions per 1,000 Beneficiaries
60
50
40
30
48.47
47.31
*CY 2010
CY 2011
20
43.92
10
0
* Calendar Year (CY)
CY 2012
12
Statewide and Regional
Readmission Data Reports
www.NoPlaceLikeHomeCA.com
13
List of Hospitals Affected by HRRP
http://www.kaiserhealthnews.org/Stories/2013/August/02/
readmission-penalties-medicare-hospitals-year-two.aspx
14
New Resource!
www.checkmypenalty.com
15
New Resource!
www.checkmypenalty.com (cont’d)
16
Home Health Quality
Improvement Campaign
http://www.homehealthquality.org/Home.aspx
17
Thank You!
Jennifer Wieckowski, MSG
Program Director, Care Transitions
jwieckowski@hsag.com
HSAG of California
700 North Brand Blvd., Suite 370
Glendale, CA 91203
818.409.9229
18
We convene providers, practitioners, and patients to
build and share knowledge, spread best practices, and
achieve rapid, wide-scale improvements in patient care;
increases in population health;
and decreases in healthcare costs for all Americans.
www.hsag.com
This material was prepared by Health Services Advisory Group of California, Inc., the Medicare Quality
Improvement Organization for California, under contract with the Centers for Medicare & Medicaid Services
(CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not
necessarily reflect CMS policy. Publication No. CA-10SOW-8.0-091813-01
19
 0
0