Research Report Biomechanics of Submaximal Recumbent Cycling in Adolescents
advertisement

Research Report
Biomechanics of Submaximal
Recumbent Cycling in Adolescents
With and Without Cerebral Palsy
Therese E Johnston, Ann E Barr, Samuel CK Lee
TE lohnston, PT, PhD, MBA, is Research Specialist, Shriners Hospitals for Children, 3551 N Broad St,
Philadelphia, PA 19140 (USA). Address all correspondence to Dr
lohnston at: tjohnstonOshrinenet.
org.
AE Barr, PT, DPT, PhD, is Associate
Professor, College of Health Professions, Temple University, Philadelphia, Pa,
SCK Lee, PT, PhD, is Research Assistant Professor, Department of
Physical Therapy, University of
Delaware, Newark, Del, and Research Associate, Shriner's Hospitals for Children,
[Johnston TE, Barr AE, Lee SCK.
Biomechanics of submaximal recumbent cycling in adolescents
with and without cerebral palsy.
Phys Ther. 2007;87:572-585,]
© 2007 American Physical Therapy
Association
Background and Purpose
The purpose of tliis study was to compare the biomechanics of recumbent cyciing
between adolescents with cerebral palsy (CP) classified at Gross Motor Function
Classification System (GMFCS) levels III and IV and adolescents with typical development (TD).
Subjects
Twent)- subjects, ages (X±SD) 15,2±1.6 years (10 with TD, 10 with CP),
participated.
Methods
Lower-extremity kinematics and muscle activity were measured at 30 and 60 rpm
while subjects pedaled on a recumbent cycle. Energy expenditure and perceived
exertion were measured during a 5-minute test, and efficiency was calculated,
Noncircular data were analyzed with analyses of variance. Circular data were analyzed using circular t tests.
Results
Differences were found between groups for joint kinematics for all motions. Subjects
with CP displayed earlier onsets and later offsets of muscle activity', increased
co-contraction of agonist and antagonist muscles, and decreased efficiency compared
with subjects with TD. There were no diffcretices in perceived exertion.
Discussion and Conclusion
Differences in cycling biomechanics between children with CP and children with TD
may be due to decreased strengtb and motor control in the children with CP.
Post a Rapid Response or
find The Bottom Line:
www.ptjournal.org
572
•
Physical Therapy
Volume 87
Number 5
May 2007
Biomechanics of Submaximai Recumbent Cycitng in Adolescents With and Wltiiout CP
C
hildren with cerebral palsy
(CF) typically have progressive impairments that affect
their function as children and later as
attults. and they have decreased fitness levels versus children with typieal development (TD). Cycling has
been stiggcsted as an inter\'ention to
address common impairments and
improve fitness levels in this population. However, little is known about
the biomecUanics of cycling in children with CP.
Ccjmpared with children with TD,
children with spastic CP have decreased muscle strength (forcegenerating capacity),' muscle spasticity (hypertoniciry).- decreased
joint range of motion (ROM),* altered motor and postural control,-*
and gait deviations.^'* Several of
these impairments are related to decreased function."" In addition, muscle co-contraction in children with
CP bas received attention during isolated liml>segment movements as
well as whole-hody activities such as
gait''"' and is a contributor to decreased motor control."
Fitness levels of people with disabUities recently have gained attention
through Healtby People 2010.'^ '* Inactivity in people with disabilities
can lead to a cycle of deconditioning, adversely affecting the cardio
vascular system, bone density, and
circulation and leading to social
isolation
and
decreased
.selfe s t e e m , " ' " Children with CP often
decline in ambulator)' status as they
become adults due to problems such
as joint pain, joint deterioration, and
overall fatigue.'" Adolescents and
adults with CP experience secondar>- conditions, including fractures,
osteoporosis. cardiova.scular system
impairments, degcnenitive joint disease, obesity, pain, contractures, depression, decreased nKjbility. dependency on otber people
for
assistance, limited opport unit it's ftjr
recreation, and st)ciai isolation.'*^
May 2007
However, most research on exercise
interventions for individuals with C;F
has focused on the younger age
groups,^" with less research directed
toward adolescents,-' a group particularly at risk for deconditioning
and potential negative health effects due to decreasing mobility that
continues into adultbood.''*-'-- In
addition, adolescents with higher
Ciross Motor Function Classification
System-^ (CiMFCS) levels and therefore decreased mobilit)' are particularly at risk as they transition from
adolescence to adulthood.
Bicycling using a moving or stationary' bicycle is a potential intervention
for cbildren with CP to address impairments while potentially minimizing joint stress,-' and studies have
begun to examine otitcomes of a
therapeutic cycling program in children with CP.^**-'' Only one study
has examined the biomechanics of
cycling in children with CP.-" A better understanding of how children
with CP cycle may help to develop
future interventions, such as volitional cycling programs or cycling
assisted by functional eleetrical stimulation. Additionally, cycling may allow children witb CP more opportunities for exercise to enbance overall
fitness, which is ciirrenth a fVicus of
the Pediatric Section of the American Physical Therapy Association.
Healthy People 2010. and the President s Council on Fitness.'^
The purpose of this study was to
determine the 3-dimensional kinematics, electromyographic (EM(i) activity, gross mechanical efficiency
(power output/metaholic inptit),-'**
and perception of effort of constantload, low-intensity stationary recumbent cycling in adolescents with CP
at GMFC:S levels III and IV compared
with tho,se of adolescents witb TD.
The hypotheses were that subjects
with CP would show increased joint
movement in the frontal and transverse planes, altered muscle activa-
tion patterns, increased muscle cocontraction around the hip and
knee, decreased gross mechanical efficiency, and greater perception of
effort during cycling compared with
subjects with TD.
Method
Subjects
Twenty adolescents participated in
the sttidy. Ten subjects (3 male, 7
female) had a diagnosis of spastic
diplegic or quadriplegic CP (age
[X±SD1 = 15,6± 1,8 years, body mass
index=24.1±4.7), and 10 subjects
(3 male, 7 female) were children
with TD (age-14,9± 1.4 years, body
mass index=22.6±5.4). Sixty percent of the subjects with CP and 40%
of the subjects with TD were fnim
minority poptilations. Subjects witb
CP were recruited from Shriners
Hospitals for Children, Philadelphia,
Pa, and subjects with TD were recruited through advertisement. Subjects 18 years of age and oldt-r and a
parent of subjects who were less
than 18 years of age signed an informed consent form approved by
the governing institutional review
board (IRB), Subjects who were less
tban 18 years of age signed an
IRB-approved assent form. All 20
screened subjects met the inclusion
and exclusion criteria for the study
(Tab. 1).
Procedure
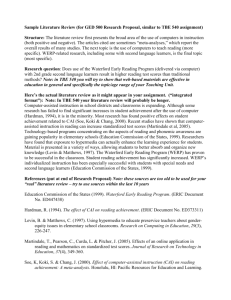
Each subject was tested while cycling on a stationary bicycle,* The
bicycle was a compact free-standing
stationary' cycle consisting of a base,
adjustable-length crank amis with adjustable pedals, handlebars, and a
control pad (Fig, 1), The pedals differed from standard hicycle pedals
by having a full footplate, atid they
differed in the location of the pedal
spindle in relation to the toot. The
pedal spindle is the point of pedal
rotation in relation to the crank arm.
• RtslonilivL-Thcrjpics Inc. 907 S
St, Builimorc, MI) 21224,
Volume 87
Number 5
Physical Therapy
•
573
Biomechanics of Submaximal Recumbent Cycling in Adolescents With and Without CP
Table 1.
Inclusion and Exclusion Criteria
Inclusion
Exclusion
Ages 13-19 y
Ability to maintain an upright sitting
pusilion with minimal suppon
Ability to commit to up to 4
sessions of training or testing
Visuopcrceptiia] skills and cognitive
and communication skills
sufficient to follow multipk-step
commands and to attend to tasks
associated with data collection
Diagnosis ol" spastic CP and
classiJifd as level III or W using
the Gross Motor Function
Classification System''
Lower-extremity onhopcdic siirger) or
traumatic fracture within the past 6 mo
Lower-extremity joint pain during cycling
Spinal fusion extending to the pelvis
Hip. knee, or ankle joint instability or
dislocation
Lower-limb stress fracttjres in the past year
Symptomatic or current diagnosis of
cardiac disease as assessed hy the
American Heart Association guidelines
for cardiac history^
Uncontrolled .seizure disorder
Current pulmonary disease or astlima and
taking oral steroids or hospitalizeti for
an acute episode in the past 6 mo
Severe spasticity in legs (score of ^ 4 on
the Modified Ashworth Scale)''
Severely limited joint range of motion or
irreversible muscle contractures that
prevented safe positioning on the cycle"
Diagnosis of athetoid or ataxic CP''
" Maron B|, Thompson PD, Puffer )C, et al. Cardiovascular preparticipation screening of competitive
athletes: a statement for health professionais from the Sudden Death Committee (clinical cardiology)
and Congenital Cardiac Defects Committee (cardiovascular disease in the young), American Heart
Association, Circulation. 1996;94:850-856.
'' Subjects with cerebral palsy (CP) only.
and the pedal spindle on a standani
bicycle pedal is located at the plantar
surface of the toot. In contrast, the
pedal spindle on the stationary' hieycle used in this study was located
closer to the lateral malleolus. The
foot was placed on a footplate that
was located 5.S cm distal to the
pedal spindle and was attached to
the pedal spindle through a metal
frame.
Because the free-standing hicyele
had no seat, suhjects were seated on
a therapy heneh^ attaehed to the
hase of the hicyele through an adjustahle bar (Fig. 1). All suhjeets plaeet!
their hands on handgrips mounted
on the sides of the bench. The speeifie ranges for adjustability of the
hack and the bar eonnecting the hieycle to the hench were determined
hy reviewing reported anthropometric data for children with TD. ages 6
to 18 years. "^ Data on children
younger than those in this study
were ineluded because children
with CP tend to be shorter and
lighter than their age-matehed peers
with TD.^"
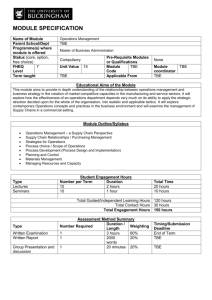
The bicycle was adjusted for each
subject individually based upon anthropometric measurements (I ig. 2).
The foot was positioned so that the
second metatarsal head was aligned
with the pedal spindle to maximi/:e
ankle power.^' This position was set
by manipulating the footplate fastened with Velero'' to the pedal. The
position of the footplate also was manipulated on the pedal to aeeommodate any lower-extremity rotational
deformities for the suhjeets with CP.
The footplate was rotated until the
knee was aligned statically in the sagittal plane. The footplate was positioned flush to the medial side of the
pedal for subjeets with TD heeause
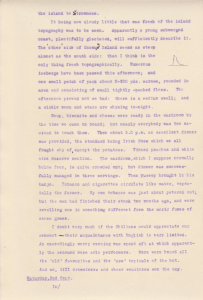
Figure 1.
Subject v^fith cerebral palsy using the cycle in the motion analysis laboratory. A therapy
bench was attached to the cycle with an adjustable bar that was set based on subject
anthropometries. The seat back was reclined 25 degrees from vertical and was heightadjustable. The reflective markers on the subject and the pedal were used for the
kinematic analysis.
574
•
Physical Therapy
Volume 87
Number 5
^ Kaye Pn>ducts, 555 Dimmwks Mill Rd, Hillshorough, NC 27278.
' Velcro tISA Inc, 406 Brown Ave, Manchester, NH 03103.
May 2007
Biomechanics of Submaximai Recumbent Cyciing in Adolescents With and Without CP
no subject with TD displayed atypical torsiona! alijinment. Subjects'
feet were .secured to tbe footplate
witb soft straps,
Eacb subject was instructed to pedal
at a cadence of 30 revolutions per
minute (rpm) and 60 rpm tising tbe
c>cle s tachometer for feedback.
Subjects wiib ID required one sbort
training session (less than !() minutes), and subjects witb CP required
1 or 2 training sessions witb a maxiiiiuni time of 20 minutes per sessiun. All subjects were permitted to
rest as needed.
Kinematic and KMG data were collected in a motion analysis laboratory. Three trials of 10 to lSsec(mds'
duration were conducted for eacb
subject for eacb cadence once tbe
targeted cadence was reacbed. Six of
the 10 subjects with CP were able to
attain and maintain 60 rpm for sbortduration trials (up to approximately
30 seconds), Tbe 4 subjects witb CP
who could not cycle at 60 rpm in the
mt)tion laboratory' could cycle at 50
qim and were tested only at this
lower cadence. The resistance load
provided during cycling was based
on each subject s weight and was
calculated using the following formula adapted from Dore et al*-: Load
(in newton-meters) = 0.49 N/kg X
body weigbt (in kilograms) x crank
arm length (in meters).
Kinematic Evaiuation
Three-tlimensional kinematics of the
bilateral bip, knee, and ankle were
collected using a 7-caniera Vicon .370
motion analysis system^ and a standard marker .set on tbe pelvis (bilateral anterior superior iliac spines and
sacrum) and tbe bilateral lower
extremities^* (Fig. 1). A rigid body
marker setup was used, and joint
centers were calculated. Data were
collected at 60 Hz and digitally fil' Vicon Motion Systems. 9 Spfctnim Pointe
Or, Lake Forest. CA 92630.
May 2007
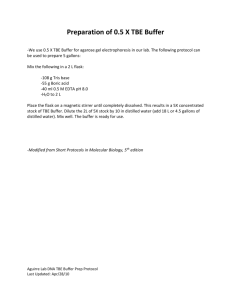
Figure 2.
Bicycle setup. Ail components were adjusted based on subject anthropometries, (1)
Seat-to-pedal distance = 85% of the distance from the greater trochanter to the base of
the calcaneus. (2) Seat-to-greater trochanter distance=15% of the distance from the
greater trochanter to the base of the calcaneus. (3) Crank arm length = 30% of tibial
length. The seat back was placed comfortably behind the subject while maintaining the
seat to greater trochanter distance.
tered using a low-pass filter of 6 Hz,
Eacb subject underwent a series of
antbropometric measures, wbicb
were required to process the kinematic data within tbe Vicon model.
A rotary encoder" mounted on tbe
crank axis recorded the crank position during eacb revolution in increments of 0.3 degree, Tbe crank arm
was calibrated in a horizontal position prior lo data collection, and 0
degrees was defined as tbe point at
wbich tbe left crank arm was borizontal and farthest trom tbe subject,
as shown in Figure 2, All data were
synchronized and processed witb
customized software using Vicon
Plug-in-Gait (Version 1.9, Build
051).^ All kinematic data were analyzed in 1-degree increments of tbe
crank position using customized
.software written in MATIJ\.B version
7.5.'
Electro myog ra p hy
Surface EMG data were collected
from 8 lower-extremity muscles (glu"tJS Digital Corp, 14(H) NE 136th Ave, ViincoiiviT. WA 9S684.
' 'nil- M:iiliW.irks Inc, 3 Apple Hill Dr, Natick,
MA 017(>()2(198.
teus maximus, rectus femoris, vastus
lateralis, medial ham.strings. biceps
femoris. anterior tibialis. lateral ga.strocnemius, and soleus) bilaterally
using standardized placement locations.^' Tbese muscles were selected
beeause tbey are major contributors
to cycling in adults.*<-'^' Tbe EMC.
data were used only to determine
muscle timing and co-contraction
during cycling.
Tbe EMG data were collected at
1,200 Hz using a Motion Lab Systems
MA-30() surface EMCi recording system," Each EMG sensor (MA-310'*)
consisted of 2 circular, stainless
steel, dry button electrode ciintacts
(12-mm diameter) tbat were preattacbed to double-differential preamplifiers IiKated witliin the electrode
housing. The EMG data were normalized across subjects by establisbing a
quiet ba.seline for each subject Ibr 6
seconds. Tbe EM(i data were digitally filtered using a band-pass filter
of 20 to 350 Hz. To tletermine the
otiset and offset of muscle activity,
EMG data were rectified and then
" Motion Lab Systems, i'i(i45 Old Hamnionil
Hwy, Baton Rouge, LA 70816-1244,
Volume 87
Number 5
Physical Therapy
•
575
Biomechanics of Submaximai Recumbent Cyciing in Adolescents With and Without CP
smoothed using a second-order lowpass Butterworth filter witb phase
correction and a cutoff frequency of
10 Hz to create a linear envelope.
The linear envelope tben was analyzed using 25-miIlisecond moving
square windows. If the mean voltage
witbin each 25-millisecond window
was at least 3 standard deviations
above tbe mean voltage during the
quiet baseline, tbe muscle was identified as being active during that time
period.^" ^" From the data, tbe crank
positions for tbe onset and offset of
muscle activity were determined
in 0.3-degree increments for eacb
muscle and eacb subject. Tbe duration of activity (in degrees) also
was calculated.
Periods of co-contraction around
each joint were identified based on
tbe percentage of the cycling revolution in wbich each of 6 agonist and
antagonist pairings around the biiateral hip and knee and tbe atikle were
co-contracting. These pairings were
the rectus femoris and biceps femoris muscles, tbe rectus femoris and
medial bam.string muscles, the vastus
lateralis and biceps femoris muscles,
tbe vastus lateralis and medial bamstring muscles, the anterior tibialis
and gastrocncmius muscles, and the
anterior tibialis and soleus muscles.
Energy Expenditure and Gross
Mechanicai Efficiency
Energy expenditure data were collected via tbe breath-by-breatb
method utilizing a SensorMedics
Vmax29 metabolic cart^^ witb subjects fasting for at least 2 bours prior
to testmg. Subjects wore a small airtigbt facemask** over tbe mouth and
nose that beld tbe flow sensor used
to measured tbe volume of oxygen
consumed (in milliliters per kilogram
of body weigbt) (Voykg) for each
breath. A gel liner** was placed inside the edges of the mask to ensure
that air passed through tbe flow sensor and did not escape around tbe
edges of the mask.
The Vo2/kg measurements were obtained under 4 consecutive conditions: (1) sitting quietly for S minutes
to establisb resting values, (2) cycling at the desired cadence for 1
minute to allow the body to warm
up. (3) cycling at the desired cadence for 5 minutes, and (4) sitting
quietly to establisb 3 minutes of recovery values. Power output data recorded once per second were dow^nloaded from customized software on
a pocket personal computer linked
to the bicycle's electronics. Following tbe test, gross mechanical efficiency was calctilated by dividing
tbe average power output (in watts)
by the average metabolic input (in
volume of oxygen consumed per kilogram of body weigbt) across the
entire 5-niinute cycling test.
Perception of Effort
Following eacb energy expenditure
testing session, subjects were asked
to rate their perception of effort using the c:bildren s OMNI Scale of Perceived Exertion.^'' There are multiple versions of the OMNI scale
depicting children doing a variety of
activities. The version used in tbis
study sbows a cbild riding a bicycle
upbill witb a score of 0 ("not tired at
all ) at the bottom of the hill and a
score of 10 ("very, very tired") at tbe
top of tbe bill and has tbe child rate
tbe exercise based on bow tired he
or sbe feels.^'-* Tbe Children's OMNI
Scale of Perceived Exertion bas been
shown to yield reliable data in a
study witb adolescent girls'" and
vahd data for cbildren ages 8 to 12
years of mixed sexes and races."
matic data were selected for analysis
for each cadence for eacb subject.
All data for the left ;md right sides
were analyzed separately, and leftand right-side data were not c<jmpared. For brevity, only the left-side
data are presented. For all data, rank
transformations usiiig normalized
ranks were performed prior to analysis secondary to a nonnormal distribution.'- A P value of less tban ,05
was accepted for significance. For
variables witb multiple measures (ie.
16 muscles), tbe accepted P value
was determined by dividing .05 by
tbat ntimber.
Kinematic data were analyzed using
3-way mixed-model analyses of variance (ANOVAs) witb crank position
used as a random factor to determine
differences in the position of tbe
joint (in degrees) based on grotip,
cadence, and crank position in
1-degree increments. The inclusion
of crank position in tbe analysis allows tbe comparison of the kinematic curves as a wbole, accotinting
for differences in joint excursions
and timing simultaneously. For FMG
data, circular / tests using t>riana
2.0^^ were performed to determine
differences in tbe crank position (in
().3-degree increments) at wbicb onset and offset of muscle activity occurred based on group and cadence.
A Mardia-Watson-Wbeeler test tising
rank transformations was used due
to tbe nonnormal distribtition of the
data,^^ A 2-way ANOVA for onset and
offset data was not performed because a model for this statistic has
not yet been developed for circulac
data. To analyze tbe duration of muscle activity\ a 2-way ANOVA basetl
on grotip and cadence was performed. Finally, an analysis of covariance (ANCOVA) based on grotip and
targeted cadence with actual cadence as a covariate was used for the
Data Anaiysis
" SensorMedics Corp, 22745 Savi Ranch Pk\,
Yorha Linda, CA 92887.
** Hans Rudolph Inc, 7200 Wyandotte, Kansas, MO 64114.
576
•
Physical Therapy
Volume 87
For kinematic and EMG analysis, 5
cycling revolutions closest to tbe targeted cadence witb complete kine-
Number 5
'* Compiiiinji Scr\'ices, 8S Nant-y-Felin Pcntnifth, Isk- of Anglesey, LL75 8tIV, Wales,
tinited Kingdom.
May 2007
Biomechanics of Submaximal Recumbent Cyciing in Adoiescents With and Without CP
Tabie 2.
Statistical Results (P Values) for the Kinematic Data"
Variable
Croup
Cadence
Crank
Position
Croup X
Cadence
Croup X
Crank Position
Croup X
Crank Position x
Cadence
Ix.'lt hip tiexion ami exteniiion
.8767
<.OOO1
<.OOO1
.0009
<.OOO1
,().-4()0
I.c-ri hip addticiion and ahdiiciion
.7649
<.OOO1
.8664
.0035
<.OOO1
,6809
l.eli hip nicdial (internal) and lateral
(external) rotaiion
.1040
<.OOO1
<.OOO1
<.32O2
<.0O01
<.OOO1
Ij;ft knee llexion and extension
.S121
<.OOO1
<.OOO1
.1722
<.OOO1
,2217
U'fl knee varus and valgus
. 1570
<.OOO1
<.OOO1
<.OOO1
<.OOO1
<.OOO1
Lffi ankle dorsitlexion and plantar flexion
. 1697
<.OOO1
<.OOO1
<.OOO1
<.OOO1
<.OOO1
" The vdlues in bold type were significant (P<.004 for significance due to 12 joint motions being studied overall). The results that include the crank position
(in degrees) reflect the comparison of the kinematic curves as a whole.
analysis of efficiency and perception
of effort due to differences in cadences achieved between groups
tluring the attempted (lO-rpm energy
expenditttre test, Tliere were no differences in achieved cadences hetween groups for tbe sborterdtiration (10-15 seconds) trials for
assessing joint kinematics and EMG
activity in tbe motion laboratory, so
an AN<X)VA was not needed for analyzing those data.
action). In tbat case, there were differences in all joint motions,
indicating tbat kinematic curves
were different. There also were differences in 3 of 6 joint motions
wbcn looking at the interaction of
group, crank position, and .speed.
Post hoc analyses were not performed for the interactions involving
the crank position dtie to tbe large
numbers of comparisons tbat would
be required, greatly reducing tbe P
value needed for significance.
Resuits
Ditlerences were seen between
groups and cadences for joint kinematics, muscle activity, and energy
expenditure dtiring cycling. As compared with subjects with TD, subjects with CV bad increased joint
movement in tbe frontal and transverse planes and altered sagittal pUuie
kinematics, Electn)m) (jgraphic activity W;LS prolonged, cocontraction was
increased, iuid efficiency was k)wer
for the subjects witb CP.
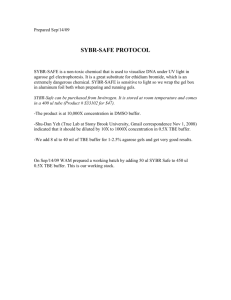
Kinematics
Figures 3 and 4 display tbe joint angles of the left lower extremity
throughout the c-ycling revolution
for each group and eacb cadence. In
additi<}n, tbere were differences between groups in the position of tbe
foot in tbe transverse plane, witb an
average of 18,8±10.'> degrees of lateral (external) rotation for subjects
with TD and 31.0± 18.0 degrees of
lateral rotation for subjects witb CP
iP=.0l5). Because the foot was
fixed to tbe footplate, minimal mcjtion was permitted in this plane.
joint kinematics of tbe left lower extremit) differed based on cadence
and crank position and interactions
involving gnjup. crank position, and
cadence (Tab. 2). No differences
were seen between groups unless
crank position was taken into account (group X crank position inter-
Subjects with CP had earlier onsets,
later offsets, and longer durations of
muscle activity for some muscles of
tbe left lower extremity compared
witb subjects witb TD (Tab. 3). Onset, offset, and duration of muscle
May 2007
E i ect ro myog ra p hy
activity for some muscles were affected by increasing cadence, witb
more activity seen at 60 rpm as compared witb 30 r^im. 1 igtire S displays
the patterns for tbe onsets and offsets of EMG activity for eacb muscle
for eacb group at eacli cadence. For
subjects witb CP cycling at 60 rpm,
average crank positions for tbe onsets and offsets of activity for tlie left
lateral gastrocnemius muscle indicate that tbe muscle was working
only briefly (Tab, 3). However, in
looking at the data for each subject,
tbe lateral gastrocnemius mtiscle
was active for most of the cycling
revolution. Therefore, the average
values do not represent the activity
of this muscie. F-igure 5 displays a
more accurate representation of tbe
activity of the lateral gaslrocnemius
muscle for the subjects with CP at 60
rpm.
In the analysis of agonist and antagonist muscle ccx'ontraction of tbe
left lower extremity, subjects with
CP had increased ct>contraction for
4 out of tbe 6 agonist and antagonist
pairings compared with subjects
with TD, atid co-contraction was
greater wben cycling at 60 rpm compared witb 30 rjim for all subjects for
4 out of the 6 pairings (Fig, 6). Stibjects with CP also had a greater increase in co-contraction witb in-
Volume 87
Number 5
Physical Therapy
•
577
Biomechanics of Submaximal Recumbent Cycling in Adoiescents With and Without CP
creasing cadence (group X cadence
interaction) compared with subjects
with TD for all 6 pairings, Bonferroni
post hoc testing showed dilfcrences
(P<.0042) in co-contraction percentage between tbe subjects witb
TD and the sttbjects witb C:P wben
cyciing at 60 rpm for all 6 significant
pairings.
Left Hip Sagittai Piane
Flex
90
85
S 80
75
70
65
0
Energy Expenditure and Cross
iVlechanicai Efficiency
30 60 90 120 150 180 210 240 270 300 330 360
Degrees
Left Hip Frontai Piane
Add
—
-12
Abd -16
1
^_^^^ i
1—
1
1
1
r——1
1
1
-TD30
CP30
TD60
CP60
1
'
1
0
30 60 90 120 150 180 210 240 270 300 330 360
Degrees
Left Hip Transverse Plane
MR
—
TD30
-CP30
TD60
CP60
Using cadence as a covariate, efficiency was greater for tbe subjects
witb TD tban for the subjects witb
CP (F=7.(>6, /'=.O127) and greater
for all subjects when cycling at 30
rpm compared with tbe attempts at
60 rpm (F=6,5I, /^=.0068) (Fig. 7),
1 here was no interaction effect of
group and cadence (F=0.41,
P=.5288). All subjects could all cycle at 30 rpm (subjects with TD at
3O.6±l.l rpm and subjects witb f.P
at 29.4±3,O rpm) throtigbout tbe energy expenditure test. However, during tbe attempted 60-rpm test, .subjects witb CP were unalilc to
maintain tbis cadence tbrotigbout
tbe test. The S .subjects witb CP who
attempted Cbe energy expenditure
test at 60 rpm cycled at 46.5±5.8
rptn, wbereas tbe subjects witb TI^
cycled at 57,9:^1,2 rpm.
Tliere were no differences between
groups (F=2.88, P=A605) or between cadences (F=5,O6, P=.U86)
180 210 240 270 300 330 360
0 30 60 90 120 150
for perceived effort as measured
Degrees
witb the Cliildren s OMNI Scale of
Figure 3.
Joint kinematics of the left hip for all subjects. Zero degrees is the point at which the left Perceived Exertion, and tbere was
(F=36.4,
crank arm was horizontal and farthest from the subject, as shown in Figure 2, Qualitative no interaction effect
differences are evident, demonstrating the differences in magnitude and timing be- /'=.3694). Subjects witb TD retween groups and cadences. Subjects with cerebral palsy (CP) had greater excursions ported median OMNI scores of 0
of motion in the frontal and transverse planes, greater hip flexion, greater knee exten- (range=0-1) and 1 (r.mge=0-6) at
sion, and greater dorsiflexion compared with the subjects with typical development
30 rpm and 60 rpm, respectively,
(TD). The positive direction indicates flexion, adduction, and medial (internal) rotation
for sagittal, frontal, and transverse planes, respectively, Flex=flexion, Add=adduction, and subjects with CP reported meAbd = abduction, MR^medial rotation, LR^Iateral (external) rotation, TD30^subjects dian (")MNI scores of 1 (range=0-6)
with TD at cadence of 30 rpm, CP30=subjects with CP at cadence of 30 rpm, and S (range=2-10) at 30 rpm and
TD60=subjects with TD at cadence of 60 rpm, CP60=subjects with CP at cadence of tbe attempted 60 rpm. respectively.
60 rpm.
With the sample size and standard
deviations in this study and witb
alpha=.O5 (2-tailed) and 80% power,
a mean score of 4.48 in tbe subjects
578
•
Physical Therapy
Volume 87
Number 5
May 2007
Biomechanics of Submaximal Recumbent Cycling in Adoiescents With and Without CP
with CP (effect size=2.38) would
bave been necessary' to attain statistical significance in OMNI scores between groups.
Left Knee Sagittal Plane
-7D30
Discussion
Differences were seen in cycling
biomecbanics between adolescents
witb CP and adolescents witb TD.
Subjects were successful with short
botits of cycling at 30 or 60 rpm in
tbis study, and no subjects were excluded from tbe study due to failure
to leam to cycle. It should be noted
that the cycle design used in tbis
study is diiferent from tbat t}'pically
used in cycling studies, and tbe results may reflect tbis specific design,
Altbougb only tbe left-side data are
presented, results for tbe right iower
extremity were overall similar to
those of the left lower extremity.
-CP30
TD60
CP60
30 60
90 120 150 180 210 240 270 300 330 360
Degrees
Left Knee Frontal Plane
Var
-TO30
-CP30
—TD60
—CP60
1
Kinematics
30 60
1
1
1
i
T
90 120 150 180 210 240 270 300 330 360
Subjects witb CP displayed differences in joint kinematics around the
bip, knee, and ankle in all 3 planes of
motion compared witb the subjects
witb TD. Altbougb tbe findings of
differences in the frotital and transverse planes were anticipated due to
differences in gait kinematics in
tbese planes,*'-^'^* differences in tbe
sagittal plane of increased hip flexion and increased knee extension for
tbe subjects with CP were unanticipated because the positioning on the
bicycle was based on antbropometrics. However, ankle dorsiflexion
was increased, tbus effectively shortening the limb, and therefore might
bave affected tbe position of tbe bip
and knee in tbe sagittal plane. Tbe
subjects with ('P may bave bad tbis
increased ankle dorsiflexion due to
decrea.sed strengtb and motor control of tbe plantar flexors,
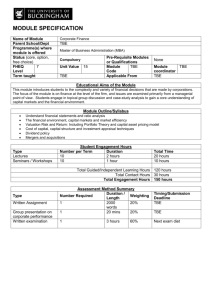
Joint kinematics of the left knee and ankle for all subjects. Zero degrees is the point at
which the left crank arm was horizontal and farthest from the subject, as shown in
Figure 2. Qualitative differences are evident, demonstrating the differences in magnitude and timing between groups and cadences. The positive direction indicates flexion
(dorsiflexion) and varus for sagittal and frontal planes, respectively, Flex^flexion,
Var=varus, Val=valgus, Df=dorsifiexion, Pf = plantar flexion. TD30=subjects with TD at
cadence of 30 rpm, CP30=subjects with CP at cadence of 30 rpm, TD60=subjects with
TD at cadence of 60 rpm, CP60=subjects with CP at cadence of 60 rpm.
Tbe differences in joint kinematics
may have been due to decreased
strengtb and motor control for tbe
subjects witb ("P. Interestingly, tbe
stibjects with CP could physically attain tbe degree of bip lateral rotation
achieved by tbe subjects witb TD,
demonstrating that ROM was not
limiting tbe ability to reach tliis joint
position. Therefore, issues sucb as
motor control and strengtb may be
May 2007
Degrees
Left Ankle Sagittai Plane
-7D30
-CP30
—TD60
—CP60
1
i
1
r
30 60 90 120 150 180 210 240 270 300 330 360
Degrees
Figure 4.
more relevant factors. Muscles can
increase or decrease the amouni of
rotation observed during functional
movements in people witb bony rotational deformities,** Thus, muscle
Volume 87
Number 5
Physical Therapy
•
579
Biomecbanics of Submaximal Recumbent Cyciing in Adoiescents With and Witbout CP
Q
_
M
»
u
i
„
~
•v
-i
fl
fl
fl
0
fO
"J
5
fj
• 1
76.4
tl
tl
r-
•0
s
tl
-?•
If
d
i~i
r-i
IN
f.
c
0
fi
tl
o i
rr,
tf l
I^
I f
-o
^
^
rf\
0 *^
*.
tn e
Q
E
Xi
• 0
tl
tl
fl
rr.
M >H
I ;
*J y 5
P
**
^
a
0t
a-.
IM
2;
"^.
oc
5.
-n
03
fl
rTJ
T j
0
•r,
fl
t--
r-t
tl
OS
rr.
=0
ir
ir>
tl
•r.
ft
p -o
~
_^
tl
up^
l-i
tl
M
"T'
OJ _0j
d
fl
ti
t-
CO
ff.
ad
if
•T
I f
X
tl
-
tl
\r-
- •
.™m in
u. o a.
0
Q. 5
£
^j
0
ago.
'4—J
Off!
V
"0
«
:ion
J 31
fi.
U
M
fl
ir
n-^
OS
•r
0
•-r
^ •
IN
fl
tl
fl
„
t-
30
3t l
+1
eu?
1--.
tl
s
tl
M.
0
rr.
r-
307.
">
83.7
tl
•!-
I
I f
tl
1
•
i• t
1
t-.
-r
•ri
ir
tl
•s
tl
1
cv
r^
u-
=>?
tl
fl
fl
I f
0
a.
E
§ 1^ £•
0
w
s
0
"
0
U
..
H
fl
fO
•*•
0
Pi
tl
9
Ol
II
1
H
Bd
•T-
SO
tl
268.
tl
fl
1
m
+1
C^
O)
r-
fl
rr.
-H
tl
—.
so
H
f-i
•r,
TO
L_
31
a
Z
u
u
i
3
3
P
•
Physical Therapy Volume 87
f
IH
i•
H
H
•
1
Number 5
ill™ S £
"S - ;
H
n
in
1
H
s
g
£
1 i
•a
(Ji
c^ c
l«l
^ -o ^
1
•
ii
1- U
580
u
B
r tibialia
i
3
u
c
dial hamstri
maxim
0
D.
(1)
c
laieralis
tion (i
M
a.
M^
IN
00
1
3
r
E
fl
—
Q
c
9.0
9.5
i
213-
Q
• ^
;
1
1
fl
242.7 92.5
W
tl
n
tl
22.1 87.1
•"
ffl
tl'
w^
•r
f'l
1
04.2
"O
V'
01
S
Qi
£
**
tl
0
255.5 36.2
°- c E
-—'
El
90.2
V
fl
VLZ
Onse , Offs(
n t
U VO
.M <n
0
257.
IJ
^
0
H
cro
92,0
1 -sfl £•0
T3
1^ !r
'Z
if-
CC
27.6
&
^ c
a
5* ft
S
•r,
—
Q
M
"5:
If
-
0
?•
o>
75.9
n
tl
1-;
tl
<*
fl
O;
h-
•'•.
•'*:
?: •• "r
U
tl
tfl
74.0
S
199
' ^ tj
50,8
c
"^
180,
11
28.
^
^ B"1
0 J!
62.1
ro
<u
u
S II
^• P
•u •
c
u
>
9 3 "^
'tj F "ra
-T
~T
ii:
IN
tl
p
~
•0
Z
-n
I f
85.
5
Tl
ai
1."
i*^
rt.
6.6
^
+1
il
...
tl'
52.
t
3.9
-gi
'8.8
x_
•p
0
III).
•0
2.7
viati(
"i
activity rather than rotational deformities may have led to some of the
differences seen. In addition, it is
possible tbat foot position altered
tbe kinematics at the more proximal
joints. The goal was to position the
foot to accommodate deformities to
allow the hip and knee to be better
aligned in the sagittal plane. Because
cycling occurs primarily in the sagittal plane, motion out of this plane
may place additional stresses on the
liip and knee joints. Further study is
needed to detennine the forces to
which these joint are exposed.
si
rf-.
r-
tl
nj
™
•I-
^
V
a 1E
•o
h:
t
X
tl
pn
•
U a e
Q
tl
•
--t
(L
1-1
IN
fi
-T
m
I f
C
* ^o
w u *
"c"
+1
tl
T
t- J
a.
W «
n ^.0
&
a
1
5,3
3
a
f 1'
15.
10
•":
^1
100,1
c
•£
n
U
fT.
>-
3
S &
® "D ' "
1^
«
f-i
'I
If
1 IL
S "5
0 5 g
E:
08.
«•
0
98.
M
a
19.6
a.
W
fl
1)9
irtl
^^
0 ,3 S
±41.7
V
i% 1^
^
TO ^
II
'j
2^
•=
£ — "D
Electromyography
Tlie EMG patterns differed for some
muscles between groups. In general,
subjects witb CP displayed earlier
onset and later offset of muscle activity within the cycling revolution
than did subjects with TD (Tab. 3,
Fig. 5). Tbese results are similar to
those of Kaplan,^" who performed a
more limited biomechanical study
comparing cycling between children
with and without C\*. Again, subjects
with CP may have experienced differences due to decreased strengtb
and motor control and therefore activated as many muscles as possible
to both stabilize the joints anti allow
movement. This pattem of increased
activity may contribute to decreased
efficiency' and greater effort during
cycling and may help to explain why
some cbildren with CP may have difficulty witb the task.
Tbere appeared to be differences in
bow subjects with TD and subjects
with CP used their muscles while
cycling. For tbe subjects witb TD,
the rectus femoris and vastus lateralis muscles appeared to act mainly as
knee extensors, whereas the subjects witb CP appeared to use tbe
rectus femoris muscle for hip flexion
in addition to using both muscles for
knee extension. Both groups appeared to use the medial hamstring
and biceps femoris muscles for a
combination of hip extension and
May 2007
Biomechanics of Submaximal Recumbent Cycling in Adolescents With and Without CP
^ 1 Extensors
^ 1 Flexors
I I No Activity
Figure 5.
Polar plots of nnean onsets and offsets of muscle activity of the left lower extremity for all subjects. Zero degrees occurred when the
left crank arnn was horizontal and farthest from the subject (Fig. 2). Muscles other than the gluteus maximus were labeled as primary
extensors and flexors based on their actions at the knee and at the ankle. The duration of activity may differ from those shown in
Table 3 because the durations here represent the difference between mean onset and mean offset. From these plots, the relationship of
activity of muscles, including co-contraction, can be seen. The innermost circle represents when hip flexion and extension occurred in order
to identify the phase. The stick figures show the approximate position of the lower extremities at that point in the revolution, and the arrow
indicates forward movement of the crank when viewed from the right side of the cycle. 1 =gluteus maximus muscle, 2 = rectus femoris
muscle, 3=vastus lateralis muscle, 4^medial hamstring muscle, 5 = biceps femoris muscle, 6=anterior tibialis muscle, 7^lateral gastrocnemius muscle, 8=soleus muscle. TD30=subjects with typical development (TD) at cadence of 30 rpm, CP30=subjects with cerebral palsy
(CP) at cadence of 30 rpm, TD60=subjects with TD at cadence of 60 rpm, CP60=subjects with CP at cadence of 60 rpm.
hip deceleration; however, for knee
flexion, subjects with TD appeared
to use the medial hamstring muscles,
whereas the subjects w^ith CP used
the hiceps femoris muscle.
May 2007
Around the ankle, subjects with TD
used the anterior tibialis muscle only
during flexion, but the subjects with
CP used tliis muscle throughout the
revolution except for a brief period
near the end ofthe extension phase.
Subjects with TD used the gastrocneniius and soleus muscles primarily
during the extension phase and into
the flexion phase at the higher ca-
Volume 87
Number 5
Physical Therapy
581
Biomechanics of Submaximal Recumbent Cycling in Adolescents With and Without CP
Percentage of Co-contraction
a,b,c
rectus/biceps rectus/mham
viat/biceps
vtat/mham
TA/gastroc
TA/sol
Figure 6.
Percentage (mean and standard deviation) of the cycling revolution in which co-contraction occurred for each agonist and antagonist
pairing around the left knee and ankle for each subject. Subjects with cerebral palsy had increased co-contraction compared with
the subjects with typical development, and all subjects displayed increased co-contraction when cycling at 60 rpm compared with
30 rpm. Rectus=rectus femoris muscle, biceps^biceps femoris muscle, vlat=vastus lateralis muscle, mham = medial hamstring
muscle, TA=anterior tibialis muscle, gastroc^gastrocnemius muscle, sol^soleus muscle. "Significant main effect of group, ^Significant main effect of cadence. 'Interaction of group and cadence. Significance defined as P<.004 due to 12 agonist and antagonist
pairings being studied (6 per side). TD30=subjects with TD at cadence of 30 rpm, CP30 = subjects with CP at cadence of 30 rpm,
TD60^subjects with TD at cadence of 60 rpm, CP60^subjects with CP at cadence of 60 rpm.
dence, potentially as a decelerator or
a knee flexor. Subjects with C;P used
these muscles primarily during the
extension phase at 30 rpm but increased the activity to nearly continuous at 60 rpm. These differences
may bave been due to poor motor
planning and the inability to dissociate the activity of some muscles, resulting in ct>contraction of muscles
around a joint. For the suhjects with
CP, it was difficult to determine
which muscle was contributing primarily to the motion observed. In
order to determine tbis, future work
would need to examine the magnitude of EMG activity.-''-^^'^^
Greater co-contraction of muscles
around the hip, knee, and ankle was
seen in subjects with CP compared
with subjects with TD. Cocontraction has been reported to occur normally during cycling in hoth
children^" and adults^' who are
healthy. The increase in cocontraction for the subjects with CP
may reflect an attempt to stabilize
582
Efficiency
n=10
n=5
TD30
CP30
TD60
CP60
Figure 7.
Cycling efficiency (mean and standard deviation) for all subjects. When actual cadence
(rather than targeted cadence) was used as a covariate, there were significant main
effects of group (P=.O127) and cadence (P=.OO68); however, the interaction was nol
significant, Vo2=volume of oxygen consumed, TD30=subjects with typical development (TD) at cadence of 30 rpm, CP30^subjects with cerebral palsy (CP) at cadence
of 30 rpm, TD60^subjects with TD at cadence of 60 rpm, CP60=subjects with CP at
cadence of 60 rpm.
Physical Therapy Volume 87 Number 5
May 2007
Biomechanics of Submaximal Recumbent Cycling in Adolescents With and Without CP
the joints wbile allowing movement
to occur. In addition, co-contraction
increased for subjects with CP when
cycling at (>() rpm compared with
cycling at 30 rpm to a greater extent
than was seen for the subjects with
ID, indicating a greater task demand
and the potential need for greater
stabilization of joints at the higher
cadence.
In this study, onset of muscle activity
was determined by EMC; amplitude
being at least 3 standard deviations
above a c|iiiet baseline. For most subjects, obtaining a quiei baseline was
not problematic; however, a quiet
baseline was unobtainable for every
muscle for every subject, which may
have undere.stimated muscle activity,
hi addition, subjects with CP often
showed constant or almost constant
activity that was 3 standard deviations above the baseline tbroughout
tlie c)cling revolution. In some of
these subjects, phasic increases in
muscle activity could be visually
identified above this level of activity,
I'herefore. the muscle activity likely
represented a combination of postural demands as well as tbe demands required for cycling. Future
work should determine tbe differences between postunil demands on
muscles versus demands for activity.
In contrast, some subjects with CP
displayed continuous, nonphasic activity throughout the cycling revolution. This finding is similar to what
was described by Kaplan,^'' who suggested Ihat the coordination of the
cycling pattern may be less affected
by continuous activit>' of some muscles due to the strength and timing of
the muscles that are acting phasically. However, this pattern may be
relatively inefficient for cycling.
In addition, subjects witb CP in
ihe present study displayed cocontraction around joints almost
continuously for some muscle combinations, especially around the anMay 2007
kle, with a greater effect at the
higher cadence. The subjects with
CP may have been using cocontraction to stabilize the foot and
ankle. Minimal dorsiflexion and
plantar-fiexion movement was noted
tor both groups. It is possible that
the pedal design used in this study
affected ankle motion, as it was a
full-length pedal in which the entire
foot maintained contact with the surface. In addition, the pedal weight
favored movement toward dorsiflexion, and the location of the pedal
spindle in relation to the foot differed. Perhaps greater stabilization
ofthe foot and ankle was required by
all subjects due to tbis pedal design,
because subjects with TD displayed
greater co-contraction around the
ankle than that reported in the literature for cycling in adults who are
healthy.*^ However, Kaplan-" reported similar percentages of cocontraction around the ankle in children with TD, as was seen with the
suhjects with TD in this study. Subjects in tbis study were adolescents, so it is unknown whether cocontraction is related to an immature
system or to pedal design. As gait
matures hefore adolescence,^*' it
would be anticipated that adolescents would bebave more like adults
while c-ycling, which recjuires a similar repetitive task but witb more
constraints to movement than with
gait.
Efficiency
Suhjects with TD cycled more efficiently than did the suhjects with
CP, and all subjects were more efficient when cycling at 30 rpm compared with cycling when attempting
60 rpm, hicreased viscous resi.stance
to motion of contracting muscle filaments'^ as well as failure of a muscle to relax between contractions
could potentially contribute to an increased metabolic cost of cycling.'"
These issues may have contributed
to a decreased efficiency for the subjects with CP due to increased met-
abolic demand. In addition, spasticity can iticrease the energy demand
due to involuntary movements, the
need to fight the spasticity in order
to move, and the need to stabilize
the hody on a cycle.'** Subjects with
CP in the present study displayed
greater muscle co-contraction than
subjects with TD, which may have
contributed to the decrease in efficiency seen in the suhjects with CP.
When attempting the 60 rpm cadence, subjects with (JP and with TD
cycled with fairly comparable efficiency (1.4±0.9 and 1.6±0.8 WM>,,
respectively) when directly comparing the values. However, although
tlie targeted cadence for each group
was the same (ie, 60 rpm), subjects
with CP had difficulty attaining and
maintaining this cadence during the
5-minute cycling test, despite heing
able to achieve this cadence during
the short trials in the motion analysis
laboratory. In addition, efficiency declines with increasing cycling cadence due to the linearly or exponentially increased demand for
oxygen.-'"'-'^' Therefore, subjects
with CP in the present study may
have cycled less efficiently if they
had been able to cycle at 60 rpm
during the S-minute cycling test.
No differences were seen between
groups or cadences in the perce(>
tion of effort as measured by the
Children's OMNI Scale of Perceived
Exertion. Unexpectedly, several subjects with CP reported a low perception of effort using the OMNI scale
during the S-minute cycling test.
Seven of the 10 subjects with CP
reported an OMNI score of 2 or less
( a little tired" or less) for the 30 rpm
test, and 1 out of 6 subjects reported
this score for the attempted 60 rpm
test. There was variability- among tbe
other subjects, with scores of 3, *),
and 6 for the remaining 3 subjects at
the 30 rpm test and scores of 5, 6,
and 10 for the remaining i subjects
during the attempted 60 rpm test.
Volume 87
Number 5
Physical Therapy
•
583
Biomechanics of Submaximal Recumbent Cycling in Adolescents With and Without CP
This variability was unanticipated
due to the similar task demand
among subjects. As the resistance
provided was based on body weight,
basing the resistance on lean body
mass or muscle volume may have
been more appropriate due to potential differences in the proportion of
fat and lean tissue among subjects.
All subjects with TD reported OMNI
scores of 0 or I at 30 rpm. There was
greater variability at 60 rpm, with 6
of the 10 .subjects reporting scores of
0 or 1, and the remaining suhjeets
reporting scores of 3, 4, 5, and 6.
Further research is needed to study lead to improvements in strength
specific outcomes, including strength- and cardiovascular conditioning in
ening and cardiovjLscular improve- adolescents with CP,
ments. Based on the results of this
study, adolescents with CP may not
This work was completed in partial fulfillbe able to cycle for longer periods of ment of the requirements for Dr )ofinston's
time due to inefficiency of tbe task. doctoral degree at Temple University,
Altbough Uiis may lead to liigher heart
authors provided concept/idea/research
rates, which are desirahle for cardio- All
design and project management. Dr
vascular benefits, it may lead to early lohnston and Dr Earr provided writing and
fatigue as well as dissatisfaction with data analysis, Dr Johnston and Dr Lee provided data collection and fund procurement,
cycling as a mode of exercise.
Dr Johnston provided subjects. Dr Lee provided facilities/equipment, Dr Barr and Dr
Lee provided institutional liaisons and consultation (including review of manuscript before submission), Dr Johnston acknowledges
her doctoral dissertation committee members Kim Nixon-Cave, PT, PhD, and Brian
Clark, PhD, as well as the following people
from Shriners Hospitals for Children who assisted in many different ways: Carrie Stackhouse, MS, Emily Slater, MS, Richard Lauer,
PhD, Brian Smith, MS, )ames McCarthy, MD,
Kyle Watson, PT, DPT, and Patricia Shewokis,
PhD (also at Drexel University). The authors
also acknowledge |ohn Caughan, PhD, of
Temple University, who assisted with the statistical analysis.
In addition, some adolescents in this
study were not able to achieve cadences higher than 30 rpm. Cycling
at this low cadence may prevent the
Training and Resistance
In this study, all subjects received attainment of a heart rate high enough
sbort training sessions, with a maxi- to achieve the cardiovascular l>enemum of 2 sessions required to ac- fits of exercise. Altered kinematics,
complish the task demands. Because pn>longed muscle activity, and cothe task and cycle design were contraction likely interfered witii tlie
novel, increased practice may have ability to cycle efficiently, and metlv
led to differences in cycling patterns, ods to encourage appropriate muscle
including joint kinematics, muscle activity may be beneficial. Extended
activity, co-contniction, and effi- training and cues such as "push out" at
ciency. With practice, co-contraction the appropriate time may lead to im- This project received funding from Shriners
may have decreased in all subjects, provements in cycling. Another pos- Hospitals for Children (grant 8530) and from
potentially leading to increased effi- sibility' is the tise of electrical stimula- a Clinical Research Grant from the Pediatric
ciency, Future work should examine tion botb as a way of providing Section of the American Physical Therapy
the changes seen with increased information on appropriate muscle Association, Dr Lee also was supported by
Institutes
of Health
grant
timing as well as to activate mus- National
practice.
HD043859.
cles to acbieve a higher cadence.
This article was received September 5, 2006,
Resistance In this study w^as based on Further research is needed to de- arid was accepted January 4, 2007.
termine
whether
techniques
such
eacb subject's body weight in order
DOI: 10.2522/pti.20060261
to allow comparison between groups. as these can be successful
However, this resistance may have
been too great for tbe subjects witb Conclusions
CP. Future work should examine cy- During cycling, adolescents witb CP References
1 Daniiimo DL, Martcllotta TL. Quintivan JM.
cling biomechanics at differing levels displayed differences in joint kineAlx-I MF, Dfficitfi in eccentric versus conof resistance to determine Its effects. matics in all 3 planes, altered muscle
centric torque in children with spiisiie (.erebral palsy, Med Sci .Sports lixetc. 201)1:
Literature on cycling in adults who activation patterns, and increased co33:117-122,
contraction
compared
with
thei
r
are healthy has shown differences in
2 Burtner PA, Quails C, Woollacott MH. IVfuscycling efficiency'^" and EMG pat- peers with TD, all of which may have
ele aciivaiLon characteristics of stance balcontrihuted
to
the
decreased
cycling
terns'*^ with differing workloads, and
ance control in children with spa,stic cerebral palsy, Cail Pasture. 1998:H:163-174,
similar effects may be seen in sub- efficiency seen In the subjects witb
3 Uleck EK Orthopedic MuHcificiiietit in CeCP, Many of the differences seen
jects witb CP.
rebnii Paisy. London, I'nitei-I Kingdom:
may be due to issues such as deMacKeith Press; \9H'^.
creased strength and motor control
4 Woollacott MH, Runner P, Neural and
Clinical Relevance
musculoskeletal eontribiilions to the deAs diiferences were seen in kinemat- for the subjects with CP. The inforvelopment of stance balance control in
typical children and in children with cea'ics, EMG, and efficiency, cycling in- mation from this study can assist in
bral palsy, Aclii PcietiiatiSit/j/tl. I W6:416:
the
development
of
future
interventerventions may provide different
18-62,
benefits for adolescents with CP tion studies, which should examine
compared with adolescents with TD. whether a cyciing intervention can
584
•
Physical Therapy
Volume 87 Number 5
May 2007
Biomechanics of Submaximai Recumbent Cyciing in Adolescents With and Without CP
5 Snssman Ml>. Cmuched gait consensus.
In: Siiisni.in Ml>. t-d. llw Di[)U'^ic Child:
hi'tjlniitioti utid Mtiriiififim-nt. Rost-mont,
111: AmtTkan Aciidt-my of Drthopacdic Sur6 Wren TA. Retliklsen S. Kay RM. Prevalence of specific gait abnomiiiliiics in chiltla'ii with txTchnil palsy: inllut-ncc of ceri'hral palsy siibiypc, age. and previitus
surHfry.y PeiluitrOrtlMi/). 2(K)S:25:79-83.
7 Damiano DL, Quinlivan J, Owen BF, ct al.
Spasticity versu.s strength in ccrebnil palsy: relationships anionj; involuntar>' resistance, voluntar)' torque, and motor function, liitrj Neuntl. 2()<)l;8(.suppl
20 Damiano DL, Vaughan CL, Abel MF. Mtiscle response to heavy resistance f xercise
in children with spastic cerebral palsy.
Der Med Chiid Neurol. 1995:37:731-739.
37 Di Fabio RP. Reliability of computerized
surface electromyogniphy for determining
the onset of mu.scle acti\ity. i'bys Wer.
1987:67:43-48.
21 Bell KJ, Oimpuu S, DeLiica PA, Romness
MJ. Natural progression of gait in children
with cerebral pals). J Pediatr Orthop.
2002:22:677-682.
38 Hodges PW, Bui IJH. A comparison of
computer-ba.sed methods for the determination of onsc-t of muscle contraction using elect romyogniphj. l-tectroencephalo^r Clin Netirophysiol. 19*X.: 101:511-519.
22 Bottos M. heliciangeli A, Sciuto L, ft al.
Functional status of adults with cerebntl
palsy and implications for treatment of
children. Dev Med Child Neurol. 2OO1;43:
516-528.
23 Palisano R, Kosenbaum P. Walter S, et al.
Development and reliability' of a system to
classify gross motor function in childa'n
with cerfbral palsy. Dev Med Child
Neurol. 1997:39:214-223.
8 Abel Mr, Damiano DI., Blanco J.S. et al, Relation.ships among nuiNculoskeletal impairmcnis and liinction:)! health status in aniliiilaior>- (trcbral palsy / Pveliatr ()rfh<>/>.
24 (iregor RJ. Fowler E. Biomeehanics of cy2OO3;2.V'>35-541.
cling. In: Zachazewski JE, Magee DJ,
9 Damiano DL, Martellotta TL. Sullivan DJ,
Qiiillf n WS, eds. Athletic Injuries and Keet al. Muscle force production and funchtihilitation. Philadelphia. Pa: WU Sauntional pertbrmance in spasiic cerehni! paldfrs Co: 1996:367-.^88.
sy: relationship ol' co-contmction Arch
25
Bloswick IXS, King EM. Brown D, et al.
Phys Med Rehabil. 2000;81:8V5-900.
Evaltiation of a device to exercise hip ex10 c;ixnna 1*, Invcmo M. Frigo C, et al. Pathotensor muscles in children with cerebral
physiological pn»tile of gait in children
palsy: a clinical and field study. Assist
with cerebral palsy. Med Spurt Sd. 1992;
Tech?iol. 1994:6:147-151.
36:186-198.
26 Physical ITierapy Clinical Research Net11 Giuliani CA. Dorsal rhizotomy for children
work. Available at: http://pt.usc.edii/
with cerebral palsy: support tor concepts
clinresnet/index.html. Accessed: August
ol motor contn)l. Pfoys lljer. 1991;7I:24824. 2{KKi.
25927 Kaplan SL. Cycling panems in children
12 Centers for Disea.se Control and Prevenwith and without cerebral palsy. Dev Med
tion and President s Council on Physical
Child Souroi. I<>95:37:62O-63O.
Fitness and Sports. Physical Activity and
28
Kston RG, Brodie DA. Responses to arm
Fitness. C^hapter 22. Healthy People
and leg ergometry. BrJ Sports Med. 19H6;
2010. US Department of Ikalth and Hu20:4-6.
man Services. 2(H)t). Available ai: http://
www.hcalthypfople.gov/Document/pdf/
29 Crawford SM. Anthropomctr). In: D<>Volumc2/22Physical.ptif. Accessed: August
cheny D, ed. Measurement in Pedititric
24, 2006.
Exercise Science. Champaign, III: Human
Kinetics Inc: 1996:17-86.
13 Centers for Disease Control and Prevention and National Institute on Disability
30 C:had KE, McKay HA, Zello (lA, et al. Body
and Rehabilitation Research, US Departcomposition in nutritionally adequate amment of Education. Disability and secbulatory and non-ambulatory children
ondary conditions, < Chapter d. Healthy
with cerebral palsy and a healthy referPeople 2010. IIS Department of Health
ence gn»up. Dev Med Child Neurol. 2()(H):
and Human Service.s. 2l)lK). Available al.
42:3.^-3.^9.
www.healthypeople.gov/Documfnt/pdt7
31
Ericson MO, Nisell R, ArixireUus UP. EkVolume l/()f>[)isability.pdf. Accessed: Auholm J. Mn.scular activity during ergomegust 24, 2006.
ter c\cling. Scand f Rehabil Med. I9H5:
14 Durstinf JL. Fainter P. I'raiiklin BA, et al.
17:53-61.
Physical activity for the chronically ill and
32
Dore
E, Bedu M, Franca NM, et al. Testing
disabled. Sports Med. 2IK)<);3O:2O7-219.
peak cycling perfomiance: effects of brak15 Lundberg A. Maximal aen)bic capacity of
ing force during growth. Med Sci Sports
young people with spastic cfrfbral palsy.
Exerc.
44
Dvv Med Child Neuml. 1978;20:205-210.
33 fJavis RB, Otmpuu S, Tyisurski D, Gage JR.
16 l-undliergA. Longitudinal .study of physical
A gait anaiysis data collection and reducworking capacity of young people with
tion technique. Hum Move Sd. 1991:20:
spa-stic cereliral palsy. Dev Med Child Neu575-587.
rol. 1984:26:328-334.
34 Jorge M. Hull ML. Analysis of EMG mea17 Rimmer JH. Physical fitness levels of per,suremfnts during bicycle pedalling./B/osons with Cfrfbral palsy. Der Med Child
mech. 1986:19:683-694.
Neurol. 2(K)l;43:2()K-2i2,
35 RaiLsih CC, Zajac FE. l,ocomotor strategy
18 Bottos M, (iericke C. Ambulatory capacity
for pedaling: muscle groups and biomein cerebnil palsy: pnignostic criteria and
chanical functions, y .VcHr(>/>/>r.s-/c)/. 1999:
consequcficfs tor intervention. Dei' .Med
82:515-525.
ChiUl Neurol. 2tK)3:'i5:7«6-79().
36 liricson MO. Muscular function during er19 Gajdosik CG, Cicirello N. Secondary congomcter cycling. Scand J Rehabil Med.
ditions of the musciilo.skcletal system in
1988;20:35-41.
adolescents and adult.s with cerebnil palsy.
Physical & Occupational Iherapy irt Pediatrics. 200l;21:49-68.
May 2007
39 Robertson RJ. Perceived Exertion for
Practitionen-i: Ratin}> liffort With tbe
l)Mi\'I Picture System. Champaign, 111: Human Kinetics Inc: 2(H)4,
40 Pfeiffer KA, Pivamik JM, Womaek CJ. et al.
Reliability and validity of the Borg and
OMNI nuing of perceived exenion scales
in adolescent girls Mvd Sci Sports Exerc.
2O02;34:2O57-2(K)l.
41 Robertson RJ. (;oss FL. Btxrr NF. et al. <:bildren s OMNI scale of perceived exertion:
mixed gender and race validation. Med Sci
Sports Exerc. 2000:32: J52-458.
42 Conover WJ, Iman RL. Rank transformations as a bridge bftwffn parametric and
nonpanimetric statistics. American .Statistician. 1981:35:124-129.
43 Sparto PJ. Schor RH. Directional statistics.
In: .Stergiou N, ed. Innovative .Analysis of
Human Mtn'emctit: Analytical Tools for
Human Movetnent Research. (Champaign.
Ul: Human Kinetics hic: 2(KI4:I21-Kil
44 Aktas S, Aiona MD, Orendurlf M Evaluation of rotational gail ahnortuality in the
patients cerebral palsy. / Pediatr Orthop.
2(MK):2O:2I7-22O.
45 Hakansson NA, Hull ML Functional roles
of the leg muscles whfn pedaling in the
recumbent versus the upright position.
J Biomech Enfi. 2(H)5:127:301-310.
46 Sutherland DH, Olshen R, Cooper L, Woo
SL. The develi>pment of mature gait.
/ Bone Joint Sur^- Am. 19«();62:3.A6'353.
47 Elliott C.r. Worthington CR Muscle contraction: viscous-like friclional forces and
the impulsive model. Inl / lUol Mucnnnol.
2OO1;29:2I3-218.
48 McDaniel J, Durstine JL, Hatld GA. Manin
JC:. Determinants of metabolic cost during
submaximal cycling. / Appt Pby.siol. 2002;
93:823-828.
49 Takaishi T, Yasuda V, Ono T, Moritani T.
Optimal pedaling rate estimated from neuromuscular fatigue for cyclists. Med Sd
Sports hixerc. 1996:28:1492-1497.
50 Hansen I-J\, Jorgensen LV. Jcnsfn K, ft al.
Cnink inertial load alTects freely chosi-n
pedal rate during cycling. J Biuniecb.
2002:35:277-285.
51 Grfgor Rl, Rugg SG, FJfects of saddle
height and pedaling cadence on power
output and efficiency, hi: Burke FR. ed.
Science of Cvclina. Champaign. Ill: Human
Kinetics Inc: 1986:69-90.
52 Bauni BS, Li L. Lower extremity nuiscic
activities during cycling are influenced by
load and iTVf\ut:ncy. J Electromyogr Kinesiol. 2003:13:181-190.
Volume 87
Number 5
Physical Therapy
585