slides
advertisement

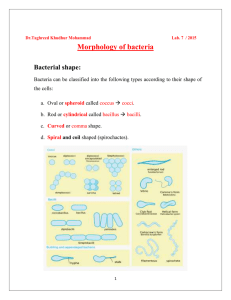
SACGR January 12, 2006 66 year old man s/p lung transplant • 66-year-old man with chronic obstructive pulmonary disease • 4 liters of oxygen at home, usually saturating around 94% • Bilateral lung transplant • Extubated POD #1 • Chest tubes pulled POD#5 • Atrial fibrillation POD#6 – started on heparin gtt • Urine Culture: GNR’s POD#6 • Increasing O2 demands 66 year old man s/p lung transplant PAST MEDICAL HISTORY 1. Chronic obstructive pulmonary disease A. FEV1 0.65. 2. Hypertension. 3. Coronary artery disease, status post stent, 12/22/2004. 4. Benign prostatic hypertrophy. 5. Hiatal hernia. PAST SURGICAL HISTORY 1. Left inguinal hernia repair in 1989. 2. Tracheotomy in January 2004 for respiratory distress secondary to car crash. 3. Tonsillectomy and adenoidectomy in childhood. MEDICATIONS ON TRANSFER 1. MMF 2. FK-506 3. Ciprofloxacin 4. Prednisone 5. Gancyclovir 6. Ampho Nebs 7. Dapsone 66 year old man s/p lung transplant ALLERGIES SULFA DRUGS. Tobacco: 55 pack-years, quit 1/04 EtOH: h/o abuse FAMILY HISTORY The patient reports type 2 diabetes on his father’s side. Reports his sister has depression and his mother has coronary artery disease. SOCIAL HISTORY Married with three daughters 66 year old man s/p lung transplant PHYSICAL EXAMINATION Temp 37.2 HR 128 BP 102/60 RR 18 SaO2 93% on RA GENERAL: alert and oriented, lying in bed. No acute distress. HEENT: Pupils are equal, round, and reactive to light and accommodation. Extraocular movements were intact. Mucous membranes moist. CHEST: crackles at bases. No rales, rhonchi or wheezes. Incision is clean, dry, and intact and well-healing. CARDIAC: tachycardic and irregularly irregular. ABDOMEN: Soft, nontender, nondistended, normal active bowel sounds. EXTREMITIES: Without clubbing, cyanosis, or edema. LABS WBC 19.7 (PMN 18) (down from 25) Hct 29 Plts 350 Na 125 K 5.4 Cl 84 HCO3 34 BUN 19 Crtn 0.9 Glc 101 INR 1.3 PTT 85 FK 8 Complications post Transplant Kotloff RM, Ahya VN, Crawford SW. Pulmonary complications of solid organ and hematopoietic stem cell transplantation. Am J Respir Crit Care Med. 2004 Jul 1;170(1):22-48. Linezolid vs Vancomycin for MRSA Pneumonia Wunderink RG, Rello J, Cammarata SK, Croos-Dabrera RV, Kollef MH. Linezolid vs vancomycin: analysis of two double-blind studies of patients with methicillin-resistant Staphylococcus aureus nosocomial pneumonia. Chest. 2003 Nov;124(5):1789-97. 66 year old man s/p lung transplant Serratia marcescens Amikacin Ampicillin Ampicillin/sulbactam Aztreonam Cefazolin Cefepime Cefotetan Ceftazidime Ceftriaxone Cefuroxime Ciprofloxacin Clindamycin Erythromycin Gentamicin Imipenem Levofloxacin Meropenem Oxacillin Piperacillin Piperacillin/tazobactam Tetracycline Tobramycin Trimeth_Sulfamethoxazole Vancomycin Staphylococcus aureus S R I S R S S S S R S S S S S S R S R R S S S S S S S Community vs Healthcare MRSA Naimi TS, LeDell KH, Como-Sabetti K, Borchardt SM, Boxrud DJ, Etienne J, Johnson SK, Vandenesch F, Fridkin S, O'Boyle C, Danila RN, Lynfield R. Comparison of community- and health care-associated methicillin-resistant Staphylococcus aureus infection. JAMA. 2003 Dec 10;290(22):2976-84. Incidence in a Children’s Hospital in Texas Risk Factors: chronic disease (50.6%), recent hospitalization (46.6%), documentedMRSAcolonization (30.7%), recent surgery (14.8%), & previous antibiotic use (11.4%). Purcell K, Fergie J. Epidemic of community-acquired methicillin-resistant Staphylococcus aureus infections: a 14-year study at Driscoll Children's Hospital. Arch Pediatr Adolesc Med. 2005 Oct;159(10):980-5. Community vs Healthcare MRSA Naimi TS, LeDell KH, Como-Sabetti K, Borchardt SM, Boxrud DJ, Etienne J, Johnson SK, Vandenesch F, Fridkin S, O'Boyle C, Danila RN, Lynfield R. Comparison of community- and health care-associated methicillin-resistant Staphylococcus aureus infection. JAMA. 2003 Dec 10;290(22):2976-84. Virulence Factors Zetola N, Francis JS, Nuermberger EL, Bishai WR. Community-acquired meticillin-resistant Staphylococcus aureus: an emerging threat. Lancet Infect Dis. 2005 May;5(5):275-86 Sub-inhibitory concentrations inhibit protein synthesis Ohlsen, K, Ziebuhr, W, Koller, KP, et al Effects of subinhibitory concentrations of antibiotics on -toxin (hla) gene expression of methicillinsensitive and methicillin-resistant Staphylococcus aureus isolates. Antimicrob Agents Chemother 1998;42,2817-2823 Sub-inhibitory concentrations inhibit protein synthesis Bernardo, K, Pakulat, N, Fleer, S, et al Subinhibitory concentrations of linezolid reduce Staphylococcus aureus virulence factor expression. Antimicrob Agents Chemother 2004;48,546-555 http://blog.hsl.washington.edu/chest/