MRSA: An Emerging Pathogen in our Community
advertisement

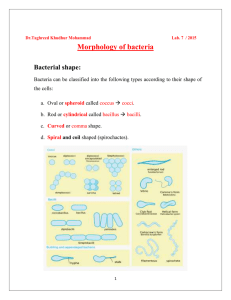
Administrative Office St. Joseph's Hospital Site, L301-10 50 Charlton Avenue East HAMILTON, Ontario, CANADA L8N 4A6 PHONE: (905) 521-6141 FAX: (905) 521-6142 http://www.fhs.mcmaster.ca/hrlmp/ Issue No. 82 QUARTERLY NEWSLETTER August 2005 MRSA: An Emerging Pathogen in our Community We have recently become aware of an increasing number of cases of skin and soft tissue infections caused by a virulent strain of Community-Acquired Methicillin-Resistant Staphylococcus aureus (CAMRSA). The first cases presented with skin abscesses and were identified from the local correctional facility in 2002. These were typed and shown to be Canadian MRSA-10, which is identical to USA 300, an organism responsible for several large outbreaks in the United States1. This organism possesses a virulence factor called the Panton Valentine Leukocidin (PVL) gene, which allows the organism to penetrate intact skin, and causes abscesses to form. Invasive infections such as necrotizing fasciitis and necrotizing pneumonia have been reported in both the United States 2,3,4 and in Canada 5. We have now identified twelve cases from the local correctional facility and many others from the community. Most of these are young patients with no known risk factors for acquiring an infection with MRSA. In all cases, treatment with a -lactam antibiotic was not effective and most required incision and drainage of the abscess. One case presented with bacteremia and rightsided endocarditis. Reports of skin and soft tissue infections in marginalized populations were presented at a Canadian Infectious Disease meeting this past April confirming that other Canadian centers are also being affected6. MRSA is universally resistant to all penicillins, cephalosporins , -lactam/-lactamase combinations and carbapenems. However, this community-acquired strain is susceptible to ciprofloxacin, trimethoprimsulfamethoxazole, rifampin, tetracycline, vancomycin and nitrofurantoin. It is generally resistant to erythromycin, but may be specifically tested, on request, to ensure susceptibility to clindamycin. Incision and drainage of the lesions usually results in clinical improvement even in the absence of appropriate antimicrobial therapy. The Hamilton Regional Laboratory Medicine Program has the ability to identify the PVL gene and to do Pulsed Field Gel Electrophoresis for typing (Figure 1) of MRSA isolated in the community. We are now offering these services to external laboratories. For questions about testing please contact Dr. Cheryl Main and the Hamilton General hospital site (905) 527-4322 ext. 46182. CA-MRSA is a virulent pathogen that is on the rise in Canada. Enhanced awareness is needed to allow rapid identification of cases, appropriate empiric therapy and prompt implementation of infection control measures. Additionally, increased surveillance is needed in order to assess the extent to which this organism has spread in the community. References 1. Miller LG, Perdreau-Remington F, Rieg G, Mehdi S, Perlroth J, Bayer AS, Tang AW, Phung TO, Spellberg B. Necrotizing fasciitis caused by community-associated methicillin-resistant Staphylococcus aureus in Los Angeles. N Engl J Med. 2005;352:1445–1453. 2. Lina G, Piémont Y, Godail-Gamot F, Bes M, Peter M, Gauduchon V, Vandenesch F, Etienne J. Involvement of Panton-Valentine Leukocidin-producing Staphylococcus aureus in primary skin infections and pneumonia. Clin Infect Dis. 1999;29:1128–1132. 3. Yamasaki O, Kaneko J, Morizane S, Akiyama H, Arata J, Narita S, Chiba J, Kamio Y, Iwatsuki K. The association between Staphylococcus aureus strains carrying Panton-Valentine Leukocidin genes and the development of deep-seated follicular infection. Clin Infect Dis. 2005;40:381–385. 4. Begier EM, Frenette K, Barrett NL, Mshar P, Petit S, Boxrud DJ, Watkins-Colwell K, Wheeler S, Cebelinski EA, Glennen A, Nguyen D, Hadler JL; Connecticut Bioterrorism Field Epidemiology Response Team. A high-morbidity outbreak of methicillinresistant Staphylococcus aureus among players on a college football team, facilitated by cosmetic body shaving and turf burns. Clin Infect Dis. 2004;39:1446–1453. 5. Mulvey MR, Chui L, Ismail J, Louie L, Murphy C, Chang N, Alfa M, and Canadian Committee for the Standardization of Molecular Methods. Development of a Canadian standardized protocol for subtyping methicillin-resistant Staphylococcus aureus using pulsed-field gel electrophoresis. J Clin Microbiol. 2001;39:3481–3485. 6. Gilbert M, Gregson D, Gillespie J, MacDonald J, Louie T, Laupland K, Louie M, Neilson D, Honish A, Hope K, Elsayed S, Zhang K, Mulvey M, Keays G, Siushansian J, Conly J. Clinical features of community-acquired Methicillin-resistant Staphylococcus aureus CA-MRSA Skin and Soft Tissue Infections (SSTI) in an outbreak in persons with histories of drug use, homelessness or incarceration. Can J Infect Dis Med Microbiol. 2005;16(2): 109. (abstract) Dr. Cheryl Main Discipline of Microbiology Hamilton Regional Laboratory Medicine Program Hamilton General Hospital Site