Vulvar & Vaginal Conditions: Overview & Diagnosis
advertisement

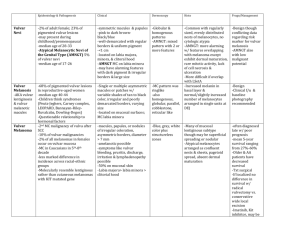
Vulva. Froberg. Katelyn Rogers. 03.03.10. Emphasis is on major characteristics & pathogenic mechs of non-neoplastic dx. Vulvar Dystrophy (bad name) Leukoplakia is better Subgroups Vulvar Neoplasms Papillary Hidradenoma Age/ occurrence Gross Any; most menopausal Smooth-surfaced, dry, stiff, white, atrophic vulva Micro Lichen sclerosus: epidermal atrophy, dermal fibrosis Squamous hyperplasia: epith thick, hyperkeratotic (now called lichen simplex chronicus - LSC) Effects Fissures, ulcers, infections, pruritis; few ca Diagnosis Biopsy!!! DDx/Rx: lichen sclerosus, lichen simplex chronicus, chronic dermatitis, Paget Disease, VIN, vulvar cancer Localized, benign, sweat gland tumor, papillae of ductal lining cells Benign Condylomas (STD- related warts) Vulvar Carcinoma Precursor: Vulvar intraepithelial neoplasia (VIN) Extramammary Paget Disease Invasive Carcinoma Accuminatum: caused by HPV Lata: symphilitic wart Some present w/ leukoplakia. Progressive grades of dysplasia I, II, II (Bowen’s dx/CIS) Presents as pruritic, red, crusted, welldelineated lesion usu on labia majora Spread pelvic & inguinal LNs Can bleed occasionally. Mimics condyloma Accuminatum: koilocytosis HPV assctd Confined to epidermis, hair follicles and sweat glands . Believed to arise from adnexal structs. Squamous cell ca = 88%. Bland Benign Concurrent vaginal &/or cervical CA in 20% Rarely assctd w/ underlying invasive cancer (as see in breast) Adenocarcinoma Melanoma Few 5% of vulvar Ca Can be up the tract, in the vagina or even in the fundus of the cervix. Sweat glands? Bartholin’s? Norm: narrow neck, cyst Chronic inflam scarring - obstructs cyst Acute inf abscess (gonococcus, Chlamydia) Norm: columnarlined, mucus-sec cyst Can form an abscess Often delayed bc embarrassed. Long survival, but may recur following surgical excision. Radical resection of vulva, pelvic + groin nodes Prog: no nodes (85% 5 y), groin nodes (66%), pelvic nodes (25%) Intraepidermal glandular cells Exophytic Fissure Carcinoma Lichen-sclerosis – atrophic adenexal struct Delay Rarely metastasizes . Cured by surgery. 30% 5 y survival Surgically drain. Inflammation Lobular papillae covered by benign epithelium. LSC Verrucous SCC Bartholin’s Gland Can be confused w/ melanoma. But PAS+ shows glands. Nests of SCC w/ keratin whorls Characteristics Vulvo-Vaginal Inflammation -Gonorrhea in kids -Trichomonas (strawberry mucosa – red) -Moniliasis (candidiasis) : white patches -Herpes (vesicles) -Senile vaginitis (drynessulcers, fissures) from decd E White fungal patches on vulva & perineum (Candida) Candida in keratin layer Congenital Lesions Imperforate hymen: -Hematocolpos (Blood filling uterus- can be irritating to peritoneum) -Reflux Septate (“double”) vagina Vaginal Adenosis Islands of cervical glds beneath squamous ectocervix cervical eruption Cause: -rarely congenital -most=maternal exposure to DES Asymp, but 0.1% clear cell adenocarcinoma In E exposure, glandular epith migrates lower into along the cervix where squamous epith is normally located. Squamous Cell Carc Precursors: Ca cervix or vulva; VIN Spread: upper vaginapelvic nodes, lower inguinal Staging: like cervix Prognosis: stage 1 = 80% 5 yr; 3-4 = <20% Adenocarcinoma Clear cell type = DESrelated Young Cancer Sarcoma Botryoides Aka. Embryonic Rhabdomyosarcom a Age: < 5yr Locally destructive; large ones metastasize Prognosis is good if txd early. Red tumor top right. Exophytic & ulcerated. Rounded, grape-like bulky mass Glycogen filled clear cells Polypoid masses, lined by squamous epith, tumor just beneathe. Atrophic glands Cambian layer of sarcoma Tichomoniasis (can also be in cervix) STD Trichomonas vaginalis Red, granular focus of vaginal adenosis w/in squamous mucosa Small blue cell tumor may show myoblastic or strap cell; striations in some Endodermal sinus (Yolk Sac) Tumor Rare ~ to same tumor in ovary Synthesizes a-FP (hyaline droplets that stain + by IHC; also inc in bld) & alpha-1-trypsin Prognosis is AWEFUL A germ cell tumor. Sheets & Schiller-Duval body (cent bld vessel surrounded by 2 layers of germ cells) Questions: For the following presentations what is the most likely diagnosis for each? Pick from the list below. Vulvar dystrophy (leukoplakia) Papillary Hidradenoma Condylomas Vulvar intraepithelial neoplasia Extramammary Paget Disease Invasive carcinoma Verrucous SCC Adenocarcinoma Melanoma Bartholin’s Gland infection Vulvo-Vaginal inflammation: gonorrhea, trichomonas, candidiasis, herpes, or senile vaginitis. Imperforate hyman Septate vagina Vaginal adenosis Squamous cell carcinoma Sarcoma Botryoides Endodermal sinus (Yolk Sac) Tumor 1. 2. 3. 4. 5. 6. Islands of cervical gland beneath squamous ectocervix leading to cervical eruption in a female whose mother was exposed to estrogens during pregnancy. This is a very rare germ cell tumor that demonstrates sheets & Schiller-Duval bodies histologically. It also has an awful prognosis. Strawberry mucosa on vaginal exam. Patient presents with leukoplaxia and level I dysplasia. She also has a history of HPV. Pruritic, red, crusted, well-delinieated lesion on labia majora. Which of these is it most important to get a biopsy in order to diagnose the cause? Answers: 1. 2. 3. 4. 5. 6. Vaginal Adenosis Endodermal sinus (Yolk Sac) Tumor Vulvo-Vaginal inflammation from trichomonas Vulvar intraepithelial neoplasia Exgtramammary Paget Disease Vulvar dystrophy (leukoplakia)