here
advertisement

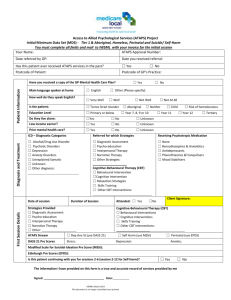
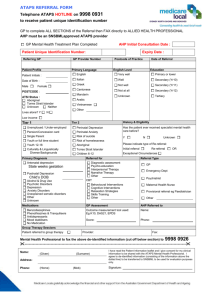
Working With Groups Under ATAPS CMHS 10th October 2013 10am-12pm PRESENTERS: Tom O’Brien FACSW Principal Psychotherapist, Mater CYMHS Senior Lecturer, School of Medicine, University of Queensland Karen Story Child and Adolescent Psychotherapist, Social Worker and Family Therapist (The Bouverie Centre ABI team). Carol Woolcock Child and Adolescent Psychotherapist and Social Worker Facilitator: Bella Saunders, Senior Psychologist APS INTRODUCTION • Groups in the ATAPS CMHS context • ATAPS CMHS Operational Guidelines: – Up to 12 group therapy services within a calendar year involving 6-10 people – Approved interventions – Evidence-based interventions. 3-Layers of Interventions Indicated Selective or Targeted Universal INDICATED INTERVENTIONS • ATAPS CMHS approved interventions are for those in the indicated and/or selective/ targeted range i.e. for those at ‘increased or higher than average risk’. • Many programs available are evidence based, however “universal” (e.g. whole class) and not group programs. WHAT IS EVIDENCE-BASED PRACTICE? • There is much debate about what defines ‘evidence-based’ practice. • A more complete definition (APA, 2005). WHICH TREATMENTS ARE EVIDENCEBASED? Useful resources: • http://www.kidsmatter.edu.au/primary/progra ms-guide/ • http://www.kidsmatter.edu.au/ec/resources/pro grams-guide/ WHY CHOOSE GROUP WORK? Group based interventions: • More cost effective than individual interventions. • More opportunity for social interaction between the participants. • More opportunity to observe the specific strengths & limitations of each participant. • Outcomes from individual interventions & group based interventions are similar. CAVEATS • Group leaders require training and supervision • It’s advisable for a new group leader to co-lead with an experienced group leader • Comprehensive assessment of each participant is required to establish needs and goals • Group selection is vital • Liaison with pre-school/ school teachers is important WHO ARE GROUPS FOR? • Children with “mild to moderate” symptoms of anxiety, depression, social withdrawal distractible/inattentive behaviour, aggression, social withdrawal & peer relationship difficulties. • Parents who can make a commitment to attend every session. WHO ARE GROUPS NOT FOR? • Children with severe externalising behaviours or severe Autism Spectrum Disorder. • Parents with untreated severe mental health problems. RESOURCES • Venue • Leaders • Materials • Back-up • Administrative assistance • Supervision Group Dynamics • Forming • Storming • Norming • Performing • Adjourning/Mourning CLINICIANS’ TIPS • Take care with group participant selection • Allow ample time to set up • Allow ample time to debrief • Practise with your co-leader • Deal with process issues as they arise • Be mindful of group dynamics • Manage your own anxiety if content is not covered. Groups with Parents WHY DO CLINICAL WORK IN GROUPS? • Normalizes the problem • Credibility – often peers have more • Peer support - inside and outside group – Group cohesion best indicator of outcome • Members can help others as well as be helped • Clinician rewards – No, not money! GROUP CBT DIFFERENT FROM INDIVIDUAL CBT? • Research evidence that Group CBT & Individual CBT have equivalent outcomes • Fundamental strategies & principles are the same • More co-therapists, more problem solvers • Process issues are where the difference lies. GROUPS WITH PARENTS OF CHILDREN 0-12 YEARS OLD • Programs that run Groups with Parents in parallel with Groups for Children • Programs that use Groups for Parents PARENT GROUPS IN PARALLEL CHILDHOOD ANXIETY, PTSD • “involving parents in treatment does provide an additional benefit, although the effects may be small” (Cresswell, C., & Cartwright-Hatton, S., 2007. Family treatment of child anxiety: Outcomes, limitations and future directions. Clinical Child and Family Psychology Review, 10, 232– 252). • learn strategies that they are able to apply in their own lives and to reflect upon the ways in which they are parenting their anxious children and whether or not these current strategies are effective… a combined parent and child traumafocused CBT condition results in the best outcomes for children (Cobham, V.E. et. al., 2012. Involving parents in indicated early intervention for childhood PTSD following accidental injury. Clinical Child and Family Psychology Review 15,345-363). PARENT TRAINING PROGRAMS BEHAVIOUR PROBLEMS, ADHD • Essentially Behavioral approaches • Triple P is local variant – Highly organized, well promoted, researched, active in training clinicians and para-professionals • “reliable positive effects of Triple P—across all settings, initial levels of problems and countries— for child behavior problems, parenting behavior, and parental well-being. There is also a strong tendency for parents’ relationship quality to improve…. Many of the present findings may be relevant to other evidence-based parenting programs.” Nowak, 2008. A comprehensive meta-analysis of Triple P. Clinical Child and Family Psychology Review. 11, 114-144. TOM’S RULES FOR GROUP THERAPISTS • Groups not (just) useful for saving time/money. They can get to places individual work can’t! • Work hard in the group but hardest outside the group (Boundary riding) – Put most effort into planning, development and recruitment of the group. – Make sure colleagues (esp. Bosses) are onside. – Liaise with referrers – Attend to dropouts, no shows and cancellations – Pre group interviews? PLANNING DILEMMAS • Groups are for patients not for clinicians – Unless they also need to be in a group • Where are the referrals going to come from? – your practice, colleagues, knowledgeable referrers • Do I need a co-therapist? • Practical arrangements – Venue, time of day, refreshments DO I REALLY NEED TO BE IN A GROUP? • Isn’t my child the problem not me? • Why do we have to air our dirty linen in front of others? • I’m not really a group kind of person • You are just trying to make more money THE GROUP IS HERE. NOW WHAT? • Program is important – Training, confidence, white coat effect. • BUT even more important – “A group is a group is a group” • Get supervision – Expert or peer. I WANT TO GET ON WITH THE PROGRAM BUT THIS PARENT JUST KEEPS BLOCKING ME? • Parent MAY have own Mental Health issues – May need you help identifying an appropriate treatment plan. • Personality styles (Personality or Group pressures?) – Dominant, Silent, Argumentative, and… • But this is where the clinical skill and experience comes in. Use it! TOM’S FINAL ADVICE • Groups can be the most rewarding part of clinical life… but also some of the toughest. • Have fun! PRE-SCHOOL GROUPS For children aged 3.5 - 6 years WHAT’S DIFFERENT? • Smaller number of participants • Activity based • Shorter group time or a break • Possibly parental interaction WHICH GROUP FOR WHOM? • Are you considering a group for children already on a ML waiting list? • Are you considering a group for a particular disorder & will gather potential participants over time? • Check the KidsMatter website for options. POSSIBLE OUTCOMES • No further intervention required • Referral for specialised assessment • Referral for further intervention -child -parent(s) HOW TO INVOLVE PARENTS • Pre-group selection interview • Transporting their child to and from the group • Information session (max 10-15 mins) at the end of each group • Consider holding an information session about half way through the group • Individual feedback sessions for each family post group DEVELOPMENTAL ISSUES Delay in fine & gross motor skills Delay in receptive & expressive language Absence of imaginative play Attachment concerns Peer relationships Some still at parallel play, others cooperative play developed • Cognitive delays • Medical conditions • • • • • • POTENTIAL DIFFICULTIES • Separation issues • Aggression between children • Tantrums GROUPS FOR CHILDREN AGED 7-11 YEARS WHICH GROUP FOR WHOM? • Are you considering a group for children already on a ML waiting list for this intervention? • Are you considering a group for a particular disorder and will gather potential participants over time? • Check the KidsMatter website for options WHICH GROUP? • Interactive groups for children & their parents are usually considered where there is a concern about the relationship. • Check the KidsMatter website for options. GROUP SELECTION • Number of participants • Need to ensure a workable group • Issue specific or a mix of issues? • Age range • Gender mix • Exclusions POSSIBLE OUTCOMES • No further intervention required • Referral for specialised assessment • Referral for further intervention -child -parent(s) HOW TO INVOLVE PARENTS • Pre-group selection interview • Transporting their child to and from the group • Consider holding an information session about half way through the group • Individual feedback sessions for each family post group. POTENTIAL DIFFICULTIES • Separating from parent • Aggression between the children • Absences from the group INTERACTIVE GROUPS Children and parents together BENEFITS OF INTERACTIVE GROUPS Opportunity for: • Leaders to observe the parent/child relationship • The parent and child to participate in enjoyable activities • Parents to practise new ways of relating to their children • Support from other parents • Learning new techniques and being coached/supported in implementation. GROUP SELECTION • Number of participants • Need to ensure a workable group • Issue specific or a mix of issues? • Age range • Gender mix • Similar socio-economic status POSSIBLE OUTCOMES • No further intervention required • Referral for specialised assessment • Referral for further intervention POTENTIAL DIFFICULTIES • Conflict between the parents • Conflict between parent and child requiring leader support & intervention • Non attendance • Possible mental health concerns in the parent QUESTIONS & ANSWERS Panel Discussion REMINDERS • Contact The ATAPS CMHS Clinical Support Service. Phone on 1800 031 185 or email clinicalsupport@psychology.org.au • Two more child mental health webinars are planned for 2013 and a further series in 2014 • A recording of the webinar will be available on the APS website shortly. See http://www.psychology.org.au/ATAPS/networking_CMHS/ • Please complete the Exit Survey – your feedback is appreciated!