ARDS: Acute Respiratory Distress syndrome The Berlin Definition of

ARDS: Acute Respiratory Distress syndrome
The Berlin Definition of ARDS
• Timing: Within 1 week of a known clinical insult or new or worsening respiratory symptoms.
• Chest imaging: Bilateral opacities on x-ray or CT scan not fully explained by effusions, lobar/lung collapse, or nodules.
• Origin of edema: Respiratory failure not fully explained by cardiac failure or fluid overload. Need objective assessment (e.g., echocardiography) to exclude hydrostatic edema if no risk factor present.
• Oxygenation:
Mild: PaO
2
/FIO
2
of 201-300 mm Hg with positive end-expiratory pressure (PEEP) or continuous positive airway pressure (CPAP) of 5 cm H
2
O or greater.
Moderate: PaO
2
/FIO
2
of 101-200 mm Hg with PEEP of 5 cm H
2
O or greater.
Severe: PaO
2
/FIO
2
of 100 mm Hg or less with PEEP of 5 cm H
2
O or greater.
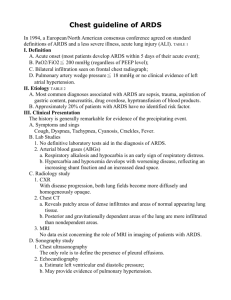
AECC consensus criteria of 1994 had
Acute onset
B/l infiltrates on CXr
Non cardiac in origin with PCWP <18mm Hg ( if swan ganz present)
P/F ratio < 300 for Acute lung injury and < 200 for ARDS
Pathologic phases of ARDS
Acute exudative phase: up to 1 week
Alveolar capillary barrier injury( damage to type 1 pneumocytes)
Development of protein rich non cardiogenic pulmonary edema
Surfactant dysfunction and deficiency( damage to type 2 cells)
Neutrophil activation and alveolar infiltration with initiation of inflammatory cascades
Pulmonary hypertension
Hyaline membrane forms
Sub acute Proliferative phase: Begins 7 days after insult
Fibroblast proliferation
Ongoing inflammation
Hyperplasia of Type 2 cells organization of hyaline membrane
Fibrosis with or without recovery; after week 3
Lungs undergo fibrosis and remodeling .Variable long term lung function.
Pathophysiology: Loss of surfactant leads to collapse and atelectasis of alveoli and also fluid influx and worsening of pulm edema
This leads to worsening lung compliance = V/P
FRC is decreased in ARDS due to alveolar edema and collapse. This results in decreased surface area for gas exchange and hypoxia.
Due to edema, collapse there is intrapulmonary shunt and low V/Q matching hypoxia
Etiology of ARDS; direct and indirect lung injury
Direct Pna, gastric aspiration, drowning
Indirect sepsis, burns, blood transfusions, and trauma
Management:
Optimize PEEP to improve FRC and hypoxia by recruitment of alveoli and redistribution of alveolar fluid into interstial space
Minimize VILI: Low tidal volume 6-8 ml/kg , permissive hypercapnia with ph.7.25, minimize 02 toxicity , Fio2,60% by optimizing peep
HFOV ; to keep lungs open at a sustained pressure
Improve O2 delivery : transfuse, correct low CO states
Fluid balance: Avoid too positive FB, worsens edema, duration of MV, LOS in PICU.
Prone position: Improves hypoxia by improving VQ matching but not overall outcomes and LOS. Greater disease in supine and more perfusion in supine thus worse V/Q, when prone, more perfusion to less diseased segments of lung thus better V/Q.
Steroids; ongoing research some benefit in adult studies
iNO: Increased PVR due to hypoxic vasoconstriction . iNO is a vasodilator and help improve V/Q matching and better because it is only pulmonary and not systemic an delivered only to those areas with gas exchange . No effect on LOS or mortality.
Exogenous surfactant: May improve some hypoxia if given early on especially in direct causes but again no change on LOS , MV etc hence not standard of care.
Rescue therapy: progressive lung failure despite maximal therapy ECMO , to be considered early in course < 7 days of MV