File - Emily Hawley
advertisement

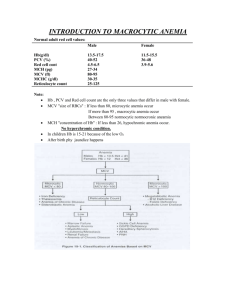
Summarize the role of folate in normal metabolism. o Folate functions include the synthesis of thymidine for DNA, the synthesis of purines for RNA, Remthylation of homocysteine to methionine, and the conversion of methionine to SAMe. Folic acid is necessary to help regulate the formation of both red and white blood cells. All of these functions are essential for protein, nucleic acid, histone, neurotransmitter, and phospholipid production. (582) Describe the digestion and absorption of folate o Folate is absorbed by intestinal conjugates that are active in the jejunum. Most is believed to occur through a sodium dependent, saturable, carrier-mediated mechanism on the brush border. Folate absorption is an energy requiring process. However when the concentration of folate increases so does passive absorption. One of the intestinal conjugates in zinc, so a zinc deficiency can also decrease folate absorption. Alcohol consumption may also decrease folate absorption and digestion. (Advanced Human Nutrition Ch. 10) List the most common causes of folate and B12 deficiencies. o Folate deficiency leads to a megaloblastic anermia, in which red blood cells are large and immature and the numbers are reduced, which in turn results in reduced oxygen carrying capacity of the blood. Individuals with the greatest risk of folate deficiency include those with chronically poor folate intake; women who have experienced multiple births; those enduring malabsorption situations, leukemia, Hodgkin disease, cancer, burns, and alcoholics. (Advanced Human Nutriton Ch, 10) o Individuals with limited amounts of B12 in their diets or who lack intrinsic factor can develop pernicious anemia. It takes many months to years to develop a deficiency because of the slow turnover. It is characterized as abnormally large, immature red blood cells. Infants have limited B12 stores, so if an infant is being fed a vegetarian based diet then they are at risk. Adults who are vegan are at a great risk as well as individuals with gastric anomalies such as gatric bypass, staping, or excessive pathology of the gastric mucosa. Those with a decreased ability to reabsorb vitamin B12 because of the low presence of IF and R proteins. 95% of deficiency cases are due to malabsorption instead of low dietary intake. (Advanced Human Nutrition Ch. 10) List all abnormal laboratory values and explain the likely cause for each abnormal value. What laboratory values or other tests support Mrs. Hicks’s diagnosis? o Mrs. Hicks had greater than normal mean cell volume, mean cell Hgb, Mean cell Hgb content, and RBC distribution. The irregular blood laboratory results are mostly due to her megaloblastic anemia from her gastric bypass. She also had lower than normal platelet count, vitamin B12, and folate. The decreased B12 and folate results are most likely due to malabsorption from the gastric bypass surgery combines with deficient dietary intake. Mrs. Hicks is diagnosed with megaloblastic anemia. What is pernicious anemia? How do these two diagnoses differ? o Pernicious anemia is a form of megaloblastic macrocytic anemia caused by the lack of intrinsic factor that leads to a vitamin B12 deficiency. (Advanced Human Nutrition Ch. 10) There is not much of a difference other than that pernicious anemia is attributed to B12 while megaloblastic anemia is attributed to folate deficiency. Identify the best dietary sources of vitamin B12 and folate. o Foods that are rich in folic acid include the following: orange juice oranges romaine lettuce spinach liver rice barley sprouts wheat germ soy beans green, leafy vegetables beans peanuts broccoli asparagus peas lentils wheat germ chick peas (garbanzo beans) o Foods rich in B12 eggs meat poultry milk shellfish fortified cereals Cited From: http://www.lpch.org/DiseaseHealthInfo/HealthLibrary/hematology/megalo b.html Assess Mrs. Hicks’s height and weight. Calculate her BMI and % usual body weight. o Height: 61 inches or 155 cm or 1.55 m o Weight: 165 # or 75 kg o BMI= 75/2.4 31.3 kg/m2 o Usual body weight: Lost 150 pounds so she used to weigh around 315 pound. o % UBW= 52% since her gastric bypass surgery Determine Mrs. Hicks’s energy and protein requirements. Explain the rationale for the methods you have used to estimate her needs. o Mifflin St. Jeor= (10 x 75) + (6.25 x 155) – (5 x 72) – 161 Energy Needs= Between 1200 and 1300 calories o Protein Requirements= 75 kg x 0.8 g/kg Protein Needs= 60 g of protein/day Identify the pertinent nutrition problems and the corresponding nutrition diagnoses o She is not in taking enough folate in her diet therefore would give her a diagnosis of inadequate vitamin intake. o altered nutrition-related laboratory values Determine your nutritional recommendations for Mrs. Hicks based on the identified nutrition problems. o Since there is a link between soft drink consumption and folate deficiency, I would recommend that Mrs. Hicks avoid consuming excessive amounts of carbonated beverages, and should be counseled against this practice. I would educated Mrs. Hicks on increasing her intake of breakfast foods fortified with folate, pyroxidine, and cobalamin. o Animal foods are the best way to improve B12 intake. Supplements of B12 don’t always work due to the pseudo B12, which is non-active in humans. (583-584) List factors that you would monitor to assess tolerance and adequacy of supplementation and dietary interventions. o Laboratory values like transcobalamin serum homocystein and serum folate levels must be consistlently monitored when she comes back for subsequent counseling sessions. Her food intake should be logged and more education about fortified foods should be continued. The absorption capacity in the GI tract is also essential for monitoring. (584)