Abdominal Pain and Vaginal Bleeding
advertisement

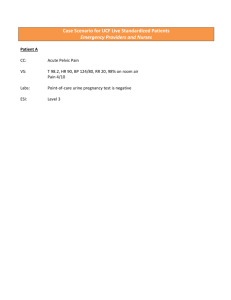
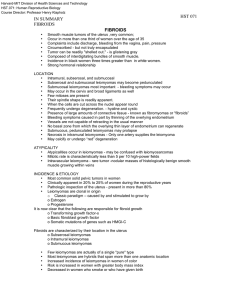
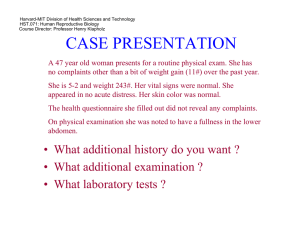
Abdominal Pain and Vaginal Bleeding HPI: C.L. is a 46 yo F G5P4 who presents with 5 days of increased vaginal bleeding and lower abdominal pain. The bleeding was spotty at first, but has increased over the past few days and is heavier than her normal period. She has passed some nickelsized blood clots. The lower abdominal pain started yesterday, is suprapubic and dull in nature without radiation. She has 6/10 pain in the ED. Her LMP was 2 weeks ago, was heavier than usual and lasted 4 days, but her cycle was normal before that. She denies any other vaginal discharge, dyspareunia or dysuria. She uses ‘the patch’ faithfully and has annual OB/GYN exams. She had some ‘weird cells’ on her last visit, but further tests were normal. She has a remote history of Chlamydia, but was ‘treated for that a long time ago’ and is in a stable monogamous relationship. C.L. feels safe at home and denies any smoking history, but does consume alcohol regularly ‘to unwind’. What else would you like to know? Current Medications: Ortho Evra, Vitamin D and Calcium, occasional Tylenol PMHx: G5P4, 1 spontaneous abortion at 12 weeks, remote history of Chlamydia, childhood asthma SocHx: non smoking, drinks alcohol regularly, no other drug use FamHx: no bleeding disorders or h/o ovarian, cervical or breast cancers. Mother – 65, living has CAD and HTN Father – deceased from MI at 62yo Siblings – 2 sisters, 30 and 35 who are healthy ROS: Gen: mild fatigue for the last 2 months HEENT: occasional headaches, no visual changes CV: denies chest pain, palpitations Resp: denies dyspnea, cough GI: no N/V/D, lower abdominal pain for 2 days, normal stools, no changes to appetite GU: vaginal bleeding x5 days, LMP 2 weeks ago, heavier than normal, denies dysuria, hematuria, dyspareunia, other vaginal discharge Skin: no rashes Neuro: denies syncope, weakness Physical Exam: Vitals: 110/65, 95, T=37.5, 98% on RA Gen: well-appearing, obese female in NAD HEENT: PERRL, EOMI, NCAT, no cervical lymphadenopathy, normal thyroid CV: RRR, no r/m/g, good peripheral perfusion Pulm: CTA, regular respirations, equal expansion Abd: mild suprapubic tenderness, non-distended, normal bowel sounds GU: normal external genitalia, moderate blood in vaginal vault coming from normal appearing multiparous cervical os, no clots, negative for cervical motion and adnexal tenderness, enlarged uterus with a smooth, rounded mass about 4 cm in diameter is palpated just below the uterine fundus, slightly left of midline Skin: normal, no rashes or lesions Neuro: normal sensation, no focal deficits Ext: normal strength and ROM What is your Differential Diagnosis? DDx: • • • • • • • • • Adenomyosis Pregnancy Ovarian tumor Endometrial polyp Endometrial cancer Leiomyosarcoma Menorrhagia Dysmenorrhea Perimenopausal What Labs/Imaging would you order next? Labs: -UPT -UA -CBC -Iron studies -PT/INR, PTT -Wet prep -GC RNA Imaging: - Abdominal Ultrasound - Pelvic Ultrasound Lab results: -UPT - negative -Wet prep - normal -GC RNA sent – results pending (will take 1-2 days for results) Urinalysis Specimen Mid stream Color Yellow Appearance Clear SpGr 1.010 pH 6.5 Protein None Glucose Negative Ketones Negative Blood 1+ WBCs/hpf 3 RBCs/hpf 5 Bacteria None Epithelial Cells/hpf None Granular casts None Waxy casts None Lab Results (continued): -CBC 9.5 8.0 300 -PT: 11 -PTT: 30 seconds MCV 68 MCHC 33 -Iron studies Iron: 33 TIBC: 475 Ferritin: 19 Transferrin Saturation: 7 Abdominal Ultrasound Imaging result: What is your diagnosis? Leiomyoma Leiomyomas (Uterine Fibroids) • Common cause of lower abdominal pain • Estrogen-dependent, uterine smooth muscle tumors • About 50% of women have leiomyomas, but only 50% are symptomatic • They may be submucosal, intramural or subserosal • They may outgrow their blood supply and degenerate or if on a pedicle can twist and become torsed. • Leiomyomas make the uterus asymmetric and enlarged and may be palpated during the physical exam Management: Initially -pain control -transfusion if Hgb <9 -patient will need iron supplementation Long term -GnRH agonists may reduce the volume of leiomyomas, but is a temporary result and reserved for pre-surgical use - Uterine embolization – IVR releases polyvinyl alcohol particles into uterine arteries causing fibroids to undergo ischemic necrosis. This procedure has unknown effects on future child bearing. - Myomectomy – removal of the uterine fibroids, for those who may still wish to bear children, however, fibroids may recur. - Hysterectomy – removal of uterus Types of Leiomyomas http://www.med.unc.edu/obgyn/specialty-services/advanced-laparoscopy-pelvic-pain/uncfibroid-center Leiomyoma - Gross Pathology Leiomyoma -Microscopic Normal myometrium is at the left, and the neoplasm is well-differentiated so that the leiomyoma at the right hardly appears different. Bundles of smooth muscle are interlacing in the tumor mass. http://library.med.utah.edu/WebPath/FEMHTML/FEM030.html Abdominal Ultrasound - Leiomyoma MRI - Leiomyoma References: 1. 2. 3. 4. Lukens TW. Chapter 100. Abdominal and Pelvic Pain in the Nonpregnant Female. In: Tintinalli JE, Stapczynski JS, Cline DM, Ma OJ, Cydulka RK, Meckler GD, eds. Tintinalli's Emergency Medicine: A Comprehensive Study Guide. 7th ed. New York: McGraw-Hill; 2011. http://www.accessmedicine.com/content.aspx?aID=6363195. Accessed December 2, 2012. Zeiger Roni F, McGraw-Hill's Diagnosaurus 2.0: http://www.accessmedicine.com/diag.aspx. Evans P. Chapter 33. Vaginal Bleeding. In: South-Paul JE, Matheny SC, Lewis EL, eds. CURRENT Diagnosis & Treatment in Family Medicine. 3rd ed. New York: McGraw-Hill; 2011. http://www.accessmedicine.com/content.aspx?aID=8154144. Accessed December 2, 2012. Shu-Huei Shen, Fiona Fennessy, Nathan McDannold, Ferenc Jolesz, Clare Tempany, Image-Guided Thermal Therapy of Uterine Fibroids, Seminars in Ultrasound, CT and MRI, Volume 30, Issue 2, April 2009, Pages 91-104, ISSN 0887-2171, 10.1053/j.sult.2008.12.002. (http://www.sciencedirect.com/science/article/pii/S0887217108001194)