Michelle-Lee Jones
Neurology PGY-3
July 15th, 2009
Coma & Brain Death - Outline
• COMA:
–
–
–
–
Definition
Pathophysiology
Aetiologies
Exam & relevant
investigations
– Differential
diagnosis &
related conditions
– Prognostication
• BRAIN DEATH:
– Definition
– Determination,
including the role
of confirmatory
testing
– Ongoing
controversies
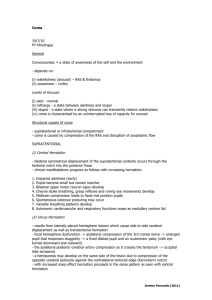
COMA
• Definition:
–Greek in origin – “deep sleep
or trance”
–It refers to an unconscious
state characterised by a lack
of both arousal and
responsiveness
COMA
• Related disorders of consciousness:
– Stupor (Latin “ to be stunned”):
aroused by and responsive to only
the most vigorous stimuli
– Minimally conscious state: Markedly
impaired consciousness with
evidence of self or environmental
awareness (intermittent rudimentary
vocal or motor responses)
COMA
• Related disorders of consciousness:
– Vegetative state: No awareness of
self or environment, but basic
cycling of arousal states & periodic
eye-opening are present
– Persistent vegetative state:
Vegetative state persisting for at
least 30 days
COMA
• Pathophysiology:
– The ascending reticular activating
system (ARAS) controls one’s level
of arousal or alertness
– The ARAS is comprised of the rostral
brainstem tegmentum (cholinergic
peribrachial nuclei*), the
diencephalon and associated cortical
projections
– *pedunculopontine tegmental nucleus & lateral dorsal
tegemental nucleus
COMA
• Pathophysiology:
– The peribrachial nuclei project via 2
major pathways – dorsal & ventral
pathways
– Dorsal: glutaminergic projections from
thalamic nuclei to various cortical areas
– Ventral: histaminergic projections from
the posterior hypothalamus (hypocretin,
orexin also) & cholinergic projections
from the basal forebrain to many cortical
areas (McGill connection Herbert Jasper 1961
& Barbara Jones 2000)
COMA
• Pathophysiology:
– Sleep centre: Preoptic area of
hypothalamus (GABAergic)
– Notably, the ARAS pathways exhibit
redundancy that may facilitate
recovery of the arousal system
(within 2-3 weeks if lesions are more
rostral)
COMA
PERIBRACHIAL NUCLEI
(http://www.nature.com/nature/journal/v437/n7063/images/nature04284f2.2.jpg)
COMA
Dorsal & Ventral ARAS pathways (Jones, B.E. 2000)
COMA
• CAVEAT: Damage to the ARAS
and associated structures or
both hemispheres is usually
necessary to cause a comatose
state. Occasionally, left
hemispheric dysfunction can per
se lead to coma...
COMA
• Aetiologies
– Structural lesions:
• Destructive & compressive
• Ischemic stroke, haemorrhage,
tumours & inflammation/infection
• Long list including SDH, EDH, SAH,
cerebral contusion, pontine
hemorrhage, cerebellar
hemorrhage/infarction, brain
abscess, vasculitis, venous sinus
thrombosis, etc.
COMA
• Aetiologies
– Herniation Syndromes:
• Munro-Kellie doctrine to consider
• Lateral displacement of the
diencephalon (e.g. basal ganglia
bleed) – monitor via displacement of
the calcified pineal gland; need 9 to
13 mm shift to produce coma;
related to initial impairment of
consciousness
COMA
• Aetiologies
– Herniation Syndromes:
• Falcine herniation –
– expanding mass causes the cingulate
gurus & pericallosal/callosomarginal
arteries to be compressed & displaced
under the falx
– Medial wall of hemisphere - infarction
& edema
– Diencephalic distortion via downward
herniation or midline shift
COMA
• Aetiologies
– Herniation Syndromes:
• Uncal hernation –
– expanding mass causes medial and
downward herniation of the medial
temporal lobe into the tentorial notch
– ipsilateral fixed & dilated pupil
– ocular dysmotility
– contralateral (uncus presses on
nearby cerebral peduncle) or
ipsilateral hemiparesis (Kernohan’s
sign)
– PCA infarction
COMA
• Aetiologies
– Herniation Syndromes:
• Central transtentorial herniation – expanding mass causes downward
herniation of the diencephalon and
pressure on the midbrain
– Ischemia & infarction as feeder
vessels are stretched and compressed
– Diabetes insipidus with pituitary stalk
avulsion
COMA
• Aetiologies
– Herniation Syndromes:
• Tonsillar herniation – Cerebellar tonsils forced down
through foramen magnum e.g. SAH
– Medullary compression apnea &
compensatory HTN
• Rostrocaudal deteriortion – downward
displacement of pons/midbrain; Duret h.
• Upward brainstem herniation
Posterior fossa lesion expands upward,
compresses dorsal midbrain
COMA
Herniation Syndromes
http://www.lfhk.cuni.cz/patfyz/I
ntranet/Figures/88/5.26.jpg
COMA
• Aetiologies
– Metabolic disturbances/toxins
• Hypoglycemia, hyperglycemic hyperosmolar
state, diabetic ketoacidosis
• Hyper/hyponatremia, hyper/hypocalemia,
hypo/hypermagnesemia, hyper/hypothroidism
• Uremic or hepatic encephalopathy
• Drugs such as alcohol, sympathomimetics,
opioids, antidepressants, salicylates, etc.
• Hypothermia, porphyria, mitochondrial
disorders
– Ischemia/Hypoxia, inflammation,
infections, seizures
COMA
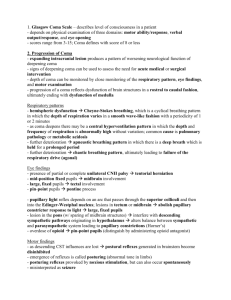
• Physical Examination &
Investigations
– General inspection: Racoon eyes, Battle sign,
hemotympanum, CSF rhinorrhea or otorrhea
basal skull fracture
– Elevated BP: hypertensive encephalopathy
(>250/150), intracerebral or subarachnoid
hemorrhage; acute ischemic infarct
– Respiratory status: Cheyne-Stokes, apneustic
breathing, atactic respiration etc.
– Hypothermia: ethanol or sedative drug
intoxication, myxedema, Wernicke
encephalopathy, hepatic encephalopathy
hypoglycemia
COMA
• Physical Examination &
Investigations
– Hyperthermia: status epilepticus, malignant
hyperthermia, anticholinergic drug intoxication,
hypothalamic lesions, pontine hemorrhage, heat
stroke
– Meningeal irritation signs for meningitis or
subarachnoid hemorrhage
– Fundoscopic exam: papilledema, retinal
hemorrhages (chronic or acute HTN); subhyaloid
(superficial retinal) hemorrhages for subarachnoid
hemorrhage
COMA
• Physical Examination &
Investigations
Pupil size, location &
reactivity
Likely site of pathology
> 7 mm, non-reactive
3rd nerve compression;
anticholinergic intox.
Slightly smaller, reactive
Early thalamic compression
Fixed midsized pupils ≈ 5 mm
Midbrain injury
Pinpoint, minimally reactive
Opioid overdose; pontine
injury, organophosphates,
neurosyphilis
COMA
• Physical Examination &
Investigations
– Oculocephalic & oculovestibular reflexes:
• If the brainstem is intact, a comatose patient
will demonstrate full conjugate horizontal eye
movements during the oculocephalic testing and
tonic conjugate movement of both eyes to the
side of the ice-water irrigation during caloric
testing.
• Absent oculovestibular responses in a comatose
patient pontine injury, sedative drug
intoxication (can also see downward deviation
of one or both eyes)
COMA
• Physical Examination & Investigations
COMA
• Physical Examination &
Investigations
– Metabolic, infectious, vasculitic, stroke W/U
– CT, MRI, EEG (mild slowing to burst
suppression – mortality rate for the latter?)
– One study found that 8% of patients
comatose secondary to brain injury are in
NCSE – role for continuous EEG monitoring
in the ICU?
COMA
• Differential Diagnosis – the
pseudocomas:
–
–
–
–
Locked-in syndrome
Akinetic mutism
Catatonia
Psychogenic unresponsiveness (which tests
can help us differentiate it from a true
coma)
– Minimally conscious
– Vegetative states
COMA - Prognostication:
AAN guidelines for coma post CPR
COMA - Prognostication
Probability of Recovering Independent Function (%)
Time Since onset of Coma (Days)
Sign
0
1
3
7
No verbal response
13
8
5
6
No eye opening
11
6
4
0
Unreactive pupils
0
0
0
0
No spontaneous eye
movements
6
5
2
0
No caloric responses
5
6
6
0
Extensor posturing
18
0
0
0
Flexor posturing
14
3
0
0
Absent motor responses
4
3
0
0
Data from Levy et al2
Prognostic Signs
in Coma from
Global Cerebral
Ischemia.
Comparison of the
Findings in Two
Studies
(Clinical Neurology, Aminoff)
Data from Edgren et
al3
No eye opening to pain
31
8
0
0
Unreactive pupils
17
7
0
0
BRAIN DEATH
• Definition:
– The irreversible loss of brain function,
inclusive of the brainstem
• Determination:
– Triad to remember: COMA, ABSENCE OF
BRAINSTEM REFLEXES (pupil, corneal,
VOR, pharyngeal & laryngeal) & APNEA
– Exclusion of confounding clinical conditions
(see table)
BRAIN DEATH
Morenski et. al , 2003
BRAIN DEATH
• Determination continued:
BRAIN DEATH
• Spontaneous and reflex movements that may be seen
in brain death:
BRAIN DEATH
• Ancillary tests:
– Transcranial doppler US
– Conventional angiography
– EEG
– Technetium-99m brain scan
– SSEPs: N20-P22 absence
bilaterally with median nerve
stimulation
Morenski et. al,
2003
A few good references
• AAN Determining Brain Death in Adults
Current guidelines
• Prediction of Outcome in Comatose
Survivors after Cardiopulmonary
Resuscitation
Current guidelines July 2006
• Plum and Posner's Diagnosis of Stupor
and Coma, 4th edition (☆☆☆☆☆) –
great book!
 0
0