Fluids and Electrolytes
advertisement

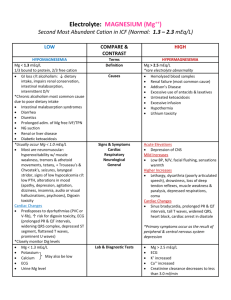
Important in o o o pts in ICU Fluids/elec can make/break a patient If give wrong fluids, pt will go down Have to be very aware of what pt has so you give him/her what they really need Thorough understanding of electrolyte metabolism Total Body Water o 50-70% of Total body weight o Male 60%; female 50% of body wt Males have more muscle --more water Females more fat; hydrophobic -- no water o Decreases with age; elderly are stooped down due to lack of water in the bones Elderly --skin not elastic anymore Elasticity comes from total amount of water In elderly, skin stays stretched or pulled o Highest proportion of tbw to body weight is found in infants Interstitial Fluid (tissues) - 15% of body wt Aldosterone - increases Na inside the intervascular space; acts as magnet to attract water from interstitial space Non functional component 1-2 % of body wt Connective tissue water -- tendons, bones, CSF CSF Joint fluid Doesn't participate in fluid exchange Na - principal extracellular cation Cl - anion o Gibbs-Donnan Equilibrium Equation Have semipermeable membrane (cell membrane); lots of movement btw intra and extra cell compartment (of ions) To have equilibrium (homeostasis), the amt of water and electrolytes on one side should always equal that of the other side; body tries to maintain that balance by movement of water and electrolytes Big molecules can't pass thru; selective membrane Hence, the majority of movement will be mostly water; some of the electrolytes will require energy to pass membrane; water diffuses freely to maintain number of ions on one side and the other If extra cell, filled with Na, water will go out to dilute amt of sodium outside o Osmotic Pressure Like a magnet The ability to attract water from one side to the other If pressure is greater in intra dept, it will attract water inside the cell If extra greater, attract water outside the cell Depends on # particles, charges, 290-310 in both compartments (intra/extra) If one becomes higher (intra), then 310 mOsm, then water comes in from outside Na acts like a magnet to the water Anything more inside/out will attract the water Total osmotic pressure Not only Na; it's Na and Cl plus magnesium, bicarbonate etc Sum of all particles found on one side of semipermeable membrane Effective Osmotic pressure Colloid oncotic pressure Pressure that attracts water from one side to the other Like osmotic pressure Normal Exchange of Fluid and Electrolytes o Know how exchange takes place o Organs Kidneys; if lots of water extracellularly, you put it out (urine output) Brain tells kidneys there's a lot of water Lungs have capacity to bring out water Skin --perspiration GIT tract or stools Water Exchange 2000-2500 ml consumed per day Daily Water Losses o Stool - 250 ml o Urine 800-1500 ml Obligatory urine loss; even if dehydrated, body will try to create urine to try to release metabolites; if don't you go into uremia ---problems to GI tract, to brain o Insensible losses -- 600 ml Losses that you can't control Obligatory loss Not lost in the form of something that you can see (water, liquid) In the form of gas --water vapor Comes from the skin and lungs Skin - 75 % (not perspiration) Lungs - 25 % Increased by hyperventilation, hypermetabolism and fever For every degree of fever above 38 degrees, add 200 ml to fluid daily losses If hyperventilating, you add another 200 ml a day (additional losses) Salt Gain and Loss o Intake -- 50-90 meq/day (3-5 g) ---one teaspoon a day only We consume much more as people Main cause of hypertension in young pts (< 35) is due to salt o Limit salt losses to < 1 meq/day In kidneys Salt-wasting- can't control amt of Na being excreted More than 200 meq maybe lost in urine; almost double your intake Sweat o o o Hypotonic loss Doesn't contain a lot of salt -- 15 meq/L If you play sports, you sweat more; drink water to prevent cramps Water has little salt; you still have cramps because you lost all the salt that water doesn't have Body fluid changes o Volume Most common problem (fluid/elec) in surgery Hypovolemia -- stab wound, bleeding, gun shot wound Volume loss -- if you have blood loss, then it's isotonic solution compared to serum --same amt of salt, Cl, Mg as other body fluids (isotonic loss); all you have is hypovolemia No exchange of water because it's volume loss Still same amt of particles in both compartments; just less volume Exchange loss with isotonic solution High sodium fluid - NSS (normal saline solution) Normal serum Na - 135-145 meq Above it --hypertonic Below -hypotonic Within- isotonic NSS - 154 meq of Na solution No potassium hypertonic Lactated Reiner's Solution 130 meq of Na (135 normal); close enough Potassium --4.5-5.5 LR -- potassium is 4 Or D5 water (no salt) No potassium MN -- normal maintenance (40 meq of Na) 14 meq of potassium Use it on special occassions Concentration If water added to fluid, concentration will change Example Person plays ball; loses water and salt; drinks purified water (no salt); reason why he gets cramp; conc of Na goes down and you don't replace it; Clinical Pt who is vomiting; Losses - potassium, Na and Cl Left at home; parents give him water Will get weaker despite water given due to loss of electrolytes Brought to hospital, check for serum electrolytes; check what's low ---usually potassium So you give MN -- it is high in potassium If low in Na, give NSS (one with highest Na) Case to case basis o Composition Can be altered without change Example Pt vomitting due to obstruction in the pylorus of stomach (has a mass); ulcer; what will he be vomitting? (water, HCl --patients lose H and Cl); initially, give pt a replacement for hydrogen which is potassium (H is cation and potassium is cation); H replaced by potassium; treat what's obstructing the stomach -- inter cell H will go out ---extracell K will go in to replace vomitus coming out; don't give IV with acid; give solution that contains 2 other cations --Na and K (both cations); only be a compostitional change; instead of H as cation, it's replaced by Na and K initially; later body will compensate for H that was lost Then you treat obstruction in the stomach o Vol changes Vol deficit - loss of fluid is not water alone Fluid replacement - LR given NGT saction diarrhea Fistula drainage Abnormal communication btw 2 epithelial lines Btw small bowel and skin Example Intestinal obstruction, TB, typhoid There's a connection btw bowel and skin What comes in, goes out Lots of effluent coming out Problematic situation not only for patient, but for surgeon Hard to treat Infections Perionitis Intestinal obstruction Burns Formula --massive losses CNS and CVS signs Tachycardia --- heart rate faster due to NE resp trying to maintain tissue perfusion (blood pressure = CO times peripheral resistance) CO = heart rate x stroke volume Tissue signs Sunken eyeballs, loss of skin turgor (elasticity lost) Oliguria -- 2ndry to renal hypoperfusion --all other organs will be sacrificied Vasoconstriction in renal artery due to angiotensin 2, endothelins Volume excess Iatrogenic One situation common; nurses try to fix fluids of pt. from 40 to 20 drops per minute; pt's will increase the fluids by themselves Extended operations (6-12 hour operations) Anastesiologist --overestimate the losses; next day you find crackles (water) in the lungs --congestive heart failure Renal Aldosterone attracts more water Liver cirrhosis Congestive heart failure Inability for heart to pump blood effectively; accumulates in the lungs Concentration Changes o Na responsible for osmolarity of the ECF comp Na -- main electrolyte that determines ECF osmolarity o Serum --tonicity o Hyponatremia Na < 130 meq (not significant) If pt who fall from 2nd floor hits his head, and serum sodium only 130; movement of water is from extra cell dept going in; little sodium; take out water -- amt of Na relative to water will increase ---- water goes into brain cell ----cells will swell and you now have edema in the brain increase in intracranial pressure To get water out of cell, give NSS -- make intracell hypertonic --now from intracell going out to extra ---to dilute excess salt you give patient ---cells will now o shrink ---avoid increase intracranial pressure --avoid brain edema Chronic hyponatremic state Asymptomatic - exhibiting/producing no symptoms until serum falls below 120 meq/L Done very slowly; if done rapidly, pt goes into seizures After surgery, due to excessive free water from breakdown of proteins, Na and fat If Na falls below 120 mEq, then you perform dialysis Hypernatremia Dry sticky mucous membrane Body temp generally elevated (almost fatal in many pts) 40-42 degree Mixed Volume Concentration o Dialysis Not done at a point when pt goes into seizures Done when you see a persistant rise in serum Na; or downfall Act before pt becomes asymptomatic High Output Renal Failure o Surgeons worry if urine output goes down (below 30 ml per hour) If happens, give more fluids, meds If you have pt who shows only signs and symp of metab Called high output renal failure Uremia occurs without… There's a rise in creatinine --metabolites not being excreted o Renal response Milder form of renal insufficiency o Seen in a state of diabetes insipitus Lots of renal output; accumulation of metabolites (not flushed out) o Treatment is dialysis Formula to compute for sodium deficit of 70 kg male with 110 meq/L Na level o 0.6 x BW (Body weight) (140 - Na) o 0.6 x 70 kg (140 -110) = 42 (.30) 1260 meq Formula to compute for potassium deficit for 60 kg female with 2 meq/l K level o 0.5 x Bw (4 - K) = 0.5 x 60 kg (4-2) = 30 (2)