Integrated Anatomy for the New
Millennium
THE NASM PERFORMANCE TEAM
Introduction
As a personal trainer, you will need to be familiar with, and in some
cases discuss, anatomy. Anatomists have developed a universally
acceptable set of reference terms that enable body structures to be
located and identified with a high degree of clarity. Without this
distinctive vocabulary, you will likely experience some confusion.
The NASM Performance Team would like to share with the health and
fitness world how traditional anatomical terminology can be functionally
applied by exploring how muscles function concentrically, eccentrically
and isometrically. Understanding how a muscle functions and interacts
through the entire muscle-action spectrum allows the personal trainer to
assess and exercise select more effectively! This article is designed to
explore the integrated function of the muscular system leading to
improved anatomical awareness, which in turn improves assessment
skills and exercise-program selection.
Why Integrated Functional Anatomy?
Traditionally, anatomy is taught topographically. It is an approach that
was developed to map the body, answer questions about our body
structures and categorize the parts. Topographic anatomy, however, is
unable to answer complex questions such as: How do the spine, pelvis,
arms and legs function as an integrated system as in real life?
Everyday function is integrated and multidimensional, not isolated.
Traditional exercises have focused on training isolated regions of the
body, often utilizing single, fixed planes of motion. For example,
functionally, the hamstrings work to eccentrically decelerate knee
extension, hip flexion and tibial internal rotation as well as assist in
concentric hip extension. The hamstrings also dynamically stabilize the
lumbo-pelvic-hip complex and the tibio-femoral joint during everyday
movements. Commonly, to strengthen the hamstrings we lay clients
prone on the hamstring curl machine and have them perform isolated,
concentric stabilized contractions without integration from the rest of the
kinetic chain (neural system, muscle system and articular system).
To break this non-functional paradigm, the health and fitness
professional must learn traditional anatomy for accurate communication
purposes and integrated anatomy for APPLICATION purposes. The
anatomical terms presented in this article enable you to assess your
understanding of anatomical terminology both traditionally and
functionally to describe the body and the interaction of its many parts.
Key muscles will be presented along with an overview of how the muscle
works concentrically, eccentrically and isometrically. For a complete
integrated anatomy review, the health and fitness professional may wish
to refer to the NASM Flashcard Series (A Comprehensive Approach to
Integrated Functional Anatomy).
INTEGRATED FUNCTIONAL ANATOMY
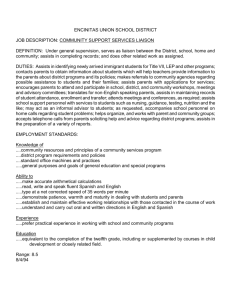
ILIOPSOAS
Traditional Function:
-Assists in concentric
acceleration of hip flexion and
hip external rotation
Integrated Function:
-Assists in eccentric
deceleration of hip extension
-Assists in eccentric
deceleration of femoral internal
rotation at heel strike
-Assists in dynamic stabilization
of the lumbo-pelvic-hip complex
during functional movements
ADDUCTOR COMPLEX
QUADRICEPS
Traditional Function:
-Assists in concentric
acceleration of femoral
adduction, flexion and
internal rotation
-The adductor magnus
assists in concentric
acceleration of hip
extension
Integrated Function:
-Assists in dynamic
stabilization of the lumbopelvic-hip complex during
functional movements
-Assists in eccentric
deceleration of femoral
abduction, extension and
external rotation
-The adductor magnus
assists in eccentric
deceleration of hip flexion
Traditional Function:
-Assists in concentric knee
and hip flexion extension
Integrated Function:
-Eccentrically decelerates
knee flexion, adduction and
internal rotation during heel
strike
-Dynamically stabilizes the
knee during functional
movement patterns
-Rectus femoris
decelerates hip extension
and knee flexion during
functional movement
patterns
ANTERIOR TIBIALIS
Traditional Function:
-Assists in concentric acceleration of ankle dorsiflexion, ankle
inversion and supination of the foot prior to heel strike
Integrated Function:
- Assists in eccentric deceleration of plantar flexion at heel strike and
eversion of the mid-foot during mid stance
- Assists in dynamic stabilization of the midtarsal joint during functional
movements
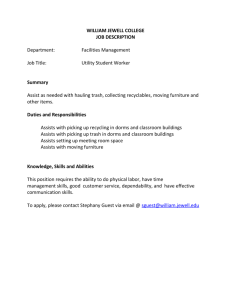
BICEPS FEMORIS
Traditional Function:
• Assists in concentric
acceleration of knee flexion,
hip extension and external
tibial rotation
Integrated Function:
• Assists in eccentric
deceleration of knee
extension, hip flexion and
internal rotation at heel strike
• Assists in eccentric
deceleration of iliosacral
anterior rotation during
functional movements
• Assists in dynamic
stabilization of the lumbopelvic-hip complex during
functional-movement
patterns
• Assists in dynamic
stabilization of the proximal
tibio-fibular joint
GLUTEUS MAXIMUS
Traditional Function:
• Concentric acceleration of
hip extension and hip
external rotation
Integrated Function:
• Eccentric deceleration of
hip flexion, hip adduction and
hip internal rotation during
the stance phase
• Assists in dynamic
stabilization of the sacroiliac
joint via the sacrotuberus
ligament and the lateral knee
via the iliotibial band
GASTROCNEMIUS
Traditional Function:
• Assists in concentric acceleration of ankle plantar flexion, knee flexion,
external rotation of the knee during propulsion and subtalar joint supination
at the end of mid-stance and is the prime mover during propulsion
Integrated Function:
• Assists in eccentric deceleration of femoral internal rotation and
deceleration of subtalar joint pronation
• Assists in dynamic stabilization of the subtalar joint and tibio-femoral joint
during transitional movements
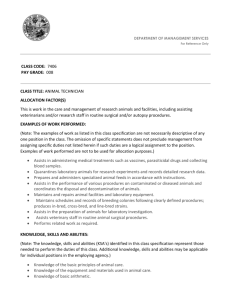
BICEPS BRACHII
PECTORALIS
MAJOR
Traditional
Function:
• Assists in
concentric
acceleration of
elbow flexion,
supination of the
radioulnar joint
and shoulder
flexion
Integrated
Function:
• Assists in
eccentric
deceleration of
elbow extension,
pronation of the
radioulnar joint
and shoulder
extension
• Assists in
dynamic
stabilization of the
humeral head
during functional
movements
Traditional
Function:
• Assists in
concentric
acceleration of
shoulder flexion,
shoulder horizontal
adduction and
internal rotation
Integrated
Function:
• Assists in
eccentric
deceleration of
shoulder extension,
horizontal abduction
and external
rotation
• Assists in dynamic
stabilization of the
shoulder complex
during overhead
movements
RECTUS ABDOMINUS
Traditional Function:
• Concentric acceleration of spinal flexion and posterior pelvic rotation
Integrated Function:
• Assists in eccentric deceleration of spinal extension, lateral flexion and
rotation and anterior pelvic rotation
• Assists in dynamic stabilization of the lumbo-pelvic-hip complex
TRAPEZIUS
Traditional Function:
• Assists in concentric acceleration of scapular elevation, scapular
retraction and depression
Integrated Function:
• Upper: Functions eccentrically to decelerate cervical flexion, lateral
flexion and rotation in addition to assisting in providing dynamic stability to
the cervical spine and shoulder complex
• Middle: Eccentrically decelerates scapular protraction and upward
rotation, assists in dynamically stabilizing the scapula during functional
movements
• Lower: Eccentrically decelerates scapular elevation, assists in
dynamically stabilizing the scapula
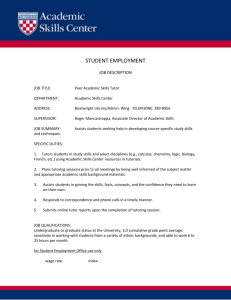
DELTOID
Traditional Function:
• Assists in concentric acceleration
of shoulder flexion, extension,
shoulder abduction, horizontal
adduction, internal and external
rotation of the shoulder
Integrated Function:
• All: Assists in dynamic
stabilization of the glenohumeral
joint during functional movements
• Assists in eccentric deceleration
of shoulder extension and external
rotation, works as a neutralizer
during shoulder abduction
• Assists in eccentric deceleration
of shoulder adduction
• Assists in eccentric deceleration
of shoulder flexion, internal rotation
and horizontal adduction, works as
a neutralizer during shoulder
abduction
LATISSIMUS DORSI
ERECTOR SPINAE
Traditional Function:
• Assists in concentric acceleration
of adduction of the humerus,
extension of the humerus and
internal rotation of the humerus
Integrated Function:
• Assists in eccentric deceleration
of abduction of the humerus,
flexion of the humerus and external
rotation of the humerus
• Assists in dynamic stabilization of
the lumbo-pelvic-hip complex
through the thoracolumbar fascia
mechanism (posterior oblique
system)
Traditional Function:
• Assists in concentric acceleration of spinal extension, spinal
rotation and lateral flexion
Integrated Function:
• Assists in eccentric deceleration of spinal flexion, spinal rotation
and lateral flexion of the lumbar spine
• Assists in dynamic stabilization of the lumbar spine during
functional movements
Conclusion
Designing an exercise program requires the health and fitness
professional to understand many interconnected training concepts. An
appreciation of the interdependence of anatomy is critical when
designing a program. All muscles function in all three planes of motion
and through the entire muscle action spectrum (eccentric, isometric,
concentric). In addition, it is evident that several muscles work
synergistically to produce force, stabilize the body and/or reduce force.
The health and fitness professional must remember that the kinetic chain
is interdependent. For example, if the anterior tibialis is weak, a client
will most likely experience increased eccentric overload to the posterior
tibialis, soleus and flexor hallucis longus as well as increased hip flexor
activity during the swing phase of gait. Increased hip flexor activity
commonly causes increased stress at the lumbo-pelvic-hip complex.
This brief example explains how a weak anterior tibialis can cause, or at
least be connected with, low back pain. Therefore, the greater the
understanding of functional anatomy, the better health and fitness
professionals can design exercise programs.
Find out more about THE NASM PERFORMANCE TEAM
Disclaimer
No warranty is given as to the accuracy of the information on any of the pages in this website. No responsibility is accepted for
any loss or damage suffered as a result of the use of that information or reliance on it. It is a matter for users to satisfy themselves
as to their or their client’s medical and physical condition to adopt the information or recommendations made. Notwithstanding a
users medical or physical condition, no responsibility or liability is accepted for any loss or damage suffered by any person as a
result of adopting the information or recommendations.
© Copyright Personal Training on the Net 1998 2003 All rights reserved