Unit 32 Assignment One 26-01
advertisement

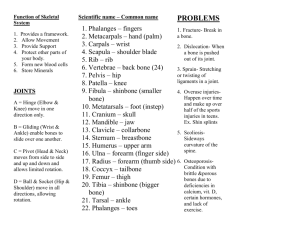
BTEC National Diploma Health Studies Unit 32 Mobility and Exercise for Health and Social Care Assignment Brief 1- Bones and Joints Tutor Name: Matthew Hopton Student Name: Clare Andrews Assignment Commencement Date: 15th September 2008 Assignment Completion Date: 12th December 2008 Clare Andrews Page 1 Matt Hopton Assignment 1 Criteria to achieve: Pass P1x P2x P3 P4x P5 P6 Merit M1x M2 M3 Distinction D1 D2 Actual Criteria Achieved: Criteria P1 Date Achieved 26-01-09 P2 26-01-09 P4 26-01-09 Tutor Signature M1 Clare Andrews Page 2 Matt Hopton TASK 1 P1, M1 On the diagram of the skeleton, clearly shade the appendicular skeleton in any colour. (Do not shade the axial skeleton) Label the bones numbered 1-24. Describe how bone shape is linked to bone function in the axial and appendicular skeletons Describe the growth and repair of bones. Analyse factors affecting growth and repair including examples of common homeostatic disorders of the skeleton and joints to help you explain the effects of different influences on skeletal development TASK 2 P2 Draw a diagram of a named synovial joint. Explain the structure and function of the three main types of joints found in the body i.e. fixed, cartilaginous and freely moveable; name at least one example of each type you have explained. Identify the six different types of synovial joint found in the body Describe the functions of the main components of a synovial joint, describe at least two disorders that may affect this joint TASK 3 P4 Describe an exercise which involves a ball and socket joint and a hinge joint (other joints may also be involved) For the exercise described, name the movements involved at the joint(s) you have mentioned. Comment upon factors which affect these movements including the muscles involved. Delivery and Assessment Windows Assignment 1 Clare Andrews Page 3 Matt Hopton Tarsal Metatarsals Phalanges Start Date Finish Date Hand In Date 15th September 2008 12th December 2008 19th January 2009 Human Skeleton Learning outcomes On completion of this unit a learner should: 1 Understand the anatomy of the musculo-skeletal system 2 Understand mechanisms of muscle contraction 3 Be able to relate balance, posture and body movement to the co-ordinated action of muscles around joints 4 Understand how common injuries and disorders of the musculo-skeletal system relate to structure and function. 1 Understand the anatomy of the musculo-skeletal system Ossification: intramembranous, endochondrial Development of skeleton: skeletal growth — lengthening of bones, closure of epiphyses, development of normal spinal curvatures (cervical, thoracic, lumbar); mineral storage, the dynamic state of bone Types of bone: histology of skeletal tissues — ligaments, tendons, cartilage, bone (compact, cancellous); structure of long bones, flat bones, bone marrow Influencing factors: genetics, age, diet, effect of weight-bearing exercise, disease Names of bones: relationship between structure, shape and function; main identifying features of — mandible and maxillae, bones of cranium, spine, girdles, limbs, chest; function of ligaments Types of joints: - moveable, eg ball and socket, hinge, gliding; synovial capsule, range of movement - immoveable, eg sutures of cranium, face, pelvis - slightly moveable — public symphysis 2 Understand mechanisms of muscle contraction Types of muscle: voluntary (skeletal); involuntary (smooth); cardiac Histological aspects: cell shape and alignment; myofibril ultrastructure — sarcomeres, actin, myosin; neuromuscular junction in voluntary muscle tissue Clare Andrews Page 4 Matt Hopton Biochemical aspects: actin, myosin; sliding filament theory — actomyosin, calcium ions, myoglobin; aerobic and anaerobic muscle contraction, fatigue, oxygen debt and recovery Mechanical aspects: movement brought about by contraction of antagonistic muscle groups; isotonic and isometric muscle contraction; stamina, suppleness, musculo-skeletal adaptations to regular exercise 3 Be able to relate balance, posture and body movement to the coordinated action of muscles around joints Named example: one of knee, hip, shoulder, elbow Movements: all those relevant to joint chosen, eg flexion, extension, adduction, abduction, circumduction, principles of antagonistic and synergistic action Muscle groups: eg quadriceps, hamstrings, calf, spinal muscles, gluteals, pectorals, abdominals, shoulder, arm Principles of levers: parts of a lever — effort, fulcrum, load; classes of lever — first class, second class, third class; examples of levers in the body, eg nodding of head, straightening of bent arm, standing on tiptoe Proprioception: spindle receptors in tendons, joints and muscles, proprioception reflexes, balance, visual input 4 Understand how common injuries and disorders of the musculoskeletal system relate to structure and function Injuries: sprain, muscle strain, fracture, dislocation, osteoarthritis, back pain, paralysis Disorders: kyphosis, scoliosis, lordosis; osteoporosis Grading criteria To achieve a pass grade the evidence must show that the learner is able to: P1 describe the structure and development of bone and the skeleton and the factors that influence it P2 explain the structure and functioning of different types of joints P3 describe the structure and contraction of different types of muscle tissue P4 explain the role of muscle groups and the principles of levers in bringing about movement around a named moveable joint P5 explain the concept of proprioception in relation to maintaining balance, posture and locomotion Clare Andrews Page 5 Matt Hopton P6 explain common injuries and disorders in relation to musculo-skeletal structure. To achieve a merit grade the evidence must show that, in addition to the pass criteria, the learner is able to: M1 explain the effect of different influencing factors on skeletal Development M2 compare the characteristics of two types of muscle in relation to their structure and functions in the body M3 explain interactions of muscle groups in maintaining posture and in locomotion of the whole body. To achieve a distinction grade the evidence must show that, in addition to the pass and merit criteria, the learner is able to: D1 analyse how musculo-skeletal functioning is affected by exercise and how exercise helps maintain healthy functioning of the musculo-skeletal system D2 use knowledge of the structure and functioning of the musculo-skeletal system to analyse the impact of common musculo-skeletal disorders on mobility and locomotion. Clare Andrews Page 6 Matt Hopton Mobility and Exercise for Health and Social Care Unit 32 Assignment One Task One - P1 There are five different types of bones within the body which all have their own specific shape which allows them to act in different ways. These consist of: Long bones Short bones Flat bones Irregular bones Sesamoid bones Long bones are hard, dense bones which are longer than they are wide. These types of bone contain yellow bone marrow and red bone marrow which produces blood cells. Long bones have a shaft, which is known as diaphysis, and two heads, which is known as epiphyses. The femur is therefore an example of a long bone as well as the tibia, fibula and humerus. This type of bone provides the body with strength, structure and mobility. Short bones are cube-shaped meaning that the length, width and height of the bone are about the same. This type of bone can be found in the carpal, which is the wrist and also in the tarsals, which is the ankle. The function of short bones is to enable the body to be able to do complex movements. Flat bones are made up of a layer of spongy bone between two thin layers of compact bone. This bone is made up of just a thin layer of bone and it is often shaped around internal organs. The shape of this bone is flattened but not Clare Andrews Page 7 Matt Hopton rounded. Flat bones also have a marrow but unfortunately not a bone marrow cavity. Examples of flat bones include the pelvic girdle, cranium and scapula. The function of flat bones is to provide the body with protection by means of forming a protective wall around internal organs. Irregular bones have a complex shape and can’t be grouped into any of the above categories. They are made up of a spongy bone which is covered with a thin layer of compact bone. Irregular bones include the vertebrae and some of the facial bones. Sesamoid bones are small bones which are located in the tendons where pressure can develop such as in the wrist. These bones can vary in numbers although the patellas are present in everyone. The process of bones forming in the body is known as ossification. The cells which are involved in the process of forming new bones are Osteoblasts and Osteocytes. Osteoblasts are known as the bone forming cells and Osteocytes are known as the mature bones cells which are from the Osteoblasts, this cell also maintains the structure of the bone. There are two types of ossification which are intramembraneous ossification and endochrondal ossification. Intramembraneous ossification is where bones develop in between layers of fibrous connective tissues to form bony tissue. Cells from the connective tissue then become Osteoblasts. Osteoblasts then produce an organic mix which makes the bones harden when calcium salts are added to this organic mix. This process is known as calcification. Endochrondal ossification involves the replacement of hyaline cartilage with bony tissue. Most of the bones in our bodies are formed in this way. In this process the Osteoblasts form a collar of compact bone around the diaphysis. At the same time, the cartilage which is located in the centre of the diaphysis begins to disintegrate and the Osteoblasts then penetrate the disintegrating cartilage and replace it with spongy bone. Ossification starts at the centre of the bones and moves towards the ends of the bones. Bones grow in length at the epiphyseal plate by a process which is similar to endochrondal ossification. The cartilage which is near to the epiphyseal plate Clare Andrews Page 8 Matt Hopton continues to grow by a process known as mitosis. The chondrocytes near to the diaphysis age and degenerate meaning the Osteoblasts move in so that they can ossify the matrix in order to form bone. This process continues throughout childhood and adolescent years up until the cartilage growth slows and stops. When cartilage growth stops, which usually occurs in the early twenties, the epiphyseal plate completely ossifies so that only a thin epiphyseal line remains and the bones can no longer grow in length. In order for bone growth to occur normally an individual needs to have: Sufficient amounts of vitamins in their diet, especially vitamin D, as this aids in the absorption of calcium. Sufficient amounts of calcium and phosphorus in their diet in order for the hardening of their bones. The right amounts of hormones being produced in their bodies including growth hormones, sex hormones, calcitonin and parathormone. The repair of bones is only needed when an individual has had some kind of surgery, broken a bone or maybe they suffer from some sort of disease where their bones can easily break. There are many different fracture types, these include: 1. A simple fracture – this is basically a clean, closed fracture. 2. A compound fracture – this break opens the skin meaning that an infection occurring could be possible. 3. A comminuted fracture – this is when the bone ends up as fragments. 4. A compression fracture – this is where all the bone becomes crushed. 5. A depressed fracture – this is where the bone is pressed inwards. 6. An impacted fracture – this is where both ends are forced into one another at the joint. 7. A spiral fracture – this is where the bone becomes twisted. 8. A greenstick fracture – this is when an incomplete break occurs. The first process which happens when repair of bones is needed is the site which is damaged Clare Andrews Page 9 Matt Hopton will bleed and become inflamed causing a blood clot to form around the injured bone, this is known as haematoma. The haematoma forms within the space which is created due to the fracturing of the bone. Next tissue repair begins with fibrocartilage filling in the space where the break occurred. Fibres which come from the protein collagen begin connect the pieces of bone. The body next receives messages, via the growth factors, that repair is required and that more cells which build the bone, known as Osteoblasts, are needed. A bony callus also forms in order to join the broken bones back together. This occurs when the Osteoblasts create a spongy bone complete with the framework, which is known as trabeculae. The last stage within repair of bones is remodelling. This is where the bone is remodelled to resemble the original bone but it however takes several months for this to happen. The Osteoblasts which create the new bones cells set up a framework of new bones cells which end up on the edges of the break. As the new cells are put in place bone-destroying cells, which are known as osteoclasts, reabsorb the spongy bone which in turn creates a medullary cavity. (Image from: http://www.apatech.com/patient-bone.html). Task Two – P2 There are many different types of joints within the body, the three main joints include: Fixed joints Cartilaginous joints Synovial joints Fixed joints within the body are joints between two bones which don’t move, for example in the skull. The plates within the skull don’t move together or against each other but they are however connected or fused. This is why fixed joints can also be known as fused joints. The bones within fixed joints are joined by fibrous connective tissue and have no joint cavity. The function of a fixed joint is to provide a protective atmosphere but they however don’t allow any growth to occur. Clare Andrews Page 10 Matt Hopton (Image from: http://assets.disaboom.com/Images/HarvardImages/102313.jpg) Cartilaginous joints within the body are joints in where the bones are tightly connected together by cartilage and where there is no joint cavity. The cartilage which is contained either contains hyaline cartilage or fibrocartilage in order to allow movements between the bones to take place. These joints only allow a little amount of movement. This type of joint can be found in the ribs and spine. The function of a cartilaginous joint is to provide the body with stability and mobility. Synovial joints are the most common and most moveable type of joint within the human body. The cavities which are located between the bones within a synovial joint are filled with synovial fluid. This fluid helps lubricate and protect the bones. The structure and function of a synovial joint differs from cartilaginous joints and fibrous joints and this is noticed quite easily. The main structural difference between synovial joints and fibrous joints is that in synovial joints there is a capsule surrounding the surfaces of the joint and that there is a synovial fluid with that capsule. This type of joint can be found in the knee. There are six different types of synovial joints within the human body. These include: Ball and socket joint Hinge joint Pivot joint Gliding joint Saddle joint Ellipsoidal joint A ball and socket joint is the most mobile type of joint in the human body. This joint allows any movement to occur in any direction. The ball-shaped head of one bone fits into a cup-like depression (socket) in another bone. This then allows flexion/extension, abduction/adduction and rotation. This type of joint can be found in the hips and shoulders. Clare Andrews Page 11 Matt Hopton Hinge joints allow movement which is similar to the opening and closing of a hinged door. This joint allows extension and retraction of an appendage. Hinge joints occur at the elbow, knee and ankle. Pivot joints allow rotation around an axis. Pivot joints occur between the atlas and axis, which is the first two vertebrae, and also between the radius and ulna. An example of a pivot joint is in the neck as this allows us to turn our head from side to side. Gliding joints are when surfaces of the bones are flat which allows side to side movements and back and forth movements. These bones are usually held together by ligaments. Gliding joints occur between carpals and tarsals. Saddle joints allow movement back and forth and up and down although it doesn’t allow any movement for rotation to occur like the ball and socket does. An example of a saddle joint is the thumb. Ellipsoidal joints are similar to a ball and socket joint. They allow the same type of movement but with lesser magnitude. This type of joint can be found in the wrist. Ellipsoidal joints can also be known as Condyloid joints. The main components of a synovial joint are: Periosteum Ligament Joint cavity Articular cartilage Fibrous capsule and the synovial membrane which are located within the articular capsule The periosteum is a membrane which has several cell layers which covers almost all of the bone. The only parts of the bone which this doesn’t cover are the parts covered by cartilage. Along with covering the bone, it also shares some of its blood supply with the bone and it produces bone when it is stimulated appropriately. Blood vessels pass from the periosteum into the Clare Andrews Page 12 Matt Hopton bone so that they can provide nutrients and oxygen as well as removing wastes and transporting newly created blood cells. The function of the ligament within a synovial joint is to hold the bones together. The ligaments are constructed from connective tissue and tend to be quite tough. This connective tissue may be located either outside the joint or in the joint cavity. The joint cavity is an enclosed space which surrounds the two articulating surfaces; it also contains the synovial fluid. The joint cavity is surrounded by a joint capsule. The articular cartilage is the thick, whitish covering of the end of the bone. The cartilage is very smooth and provides the sliding surface of the joint. This cartilage covers surfaces of articulating bones however it doesn’t bind these together. The function of the articular cartilage is to hold together the ends of the bones which form the joints and to also support the delicate inner layer which is the synovial membrane. The articular capsule surrounds the articular surfaces as well as enclosing the joint cavity. Within the articular capsule are the fibrous capsule and the synovial membrane. The fibrous capsule is the outer layer of the articular capsule and this is attached to the periosteum of bones. It is also composed of collagen. The synovial membrane is the inner layer of the articular capsule in where the synovial fluid is found. The function of the fluid is to cushion the joint and protect the ends of the bones from grating on one another. It also provides nourishment for the articular cartilage. Osteoarthritis is a disorder which can affect the synovial joint. Osteoarthritis affects an individual’s joints and is the most common condition to affect synovial joints. With this condition, the ends of the joints, which are covered in cartilage, degenerate causing bone to rub against bone. The cartilage then becomes worn and uneven due to this and causes the bones to get thicker and broader. Osteophytes, which are bony outgrowths, can also form within Clare Andrews Page 13 Matt Hopton this area and this in turn may lead to pain, stiffness and loss of function in the area at times. Osteoarthritis also causes mild inflammation of the tissues around the joints, known as synovitis. If an individual has osteoarthritis in their knees it is likely that both their knees will be affected and so therefore this means that both the synovial joints will be affected. This may also cause fluid to build up in the joints causing them to swell up. The main symptoms of osteoarthritis are: Pain Stiffness which appears to be worst in the morning but improves within 30 minutes once the individual has started to move Difficulty moving the affected joints There are many cases of osteoarthritis in where individuals don’t suffer from any kinds of symptoms. The symptoms may begin to develop slowly and they may be experienced within one joint or a few joints. Other symptoms of osteoarthritis which aren’t as common as the others include: Warm joints Joint tenderness Weakness and muscle wasting (loss of muscle bulk) Increased pain and stiffness when an individual hasn’t moved their joints for a while. Joints appearing slightly larger, a grating or crackling sound or sensation in your joints. A limited amount of movements within the joints The treatment for osteoarthritis is usually by means of taken medication, such as paracetamol and anti-inflammatory tablets, due to the fact that osteoarthritis can’t be cured it can only be helped. Treatment for this condition can also include the use of cream, a tens machine and injections. As a last resort individuals can have surgery if their symptoms are that bad. There are not specific tests which diagnose osteoarthritis so when individuals think they may have this, their GP will ask them about there symptoms and carry out an examination of their joints. Tests such as X-rays and blood tests aren’t usually required when diagnosing osteoarthritis, however in some cases an individual’s GP may opt for the individual to have X-rays and blood tests just to rule of any possible fractures or rheumatoid arthritis. Clare Andrews Page 14 Matt Hopton Bursitis is another condition which can affect the synovial joints. A bursa is a fluid-filled sac which reduces friction around the joints. The bursa is lined with cells called synovial cells and these secrete a fluid rich in collagen and proteins. When the bursa becomes swollen due to the fluid inside being infected or irritated because of too much movement, the condition known as bursitis occurs. Bursitis causes pain, swelling and difficulty moved the joint which is affected. Bursitis can affect any joint within the body such as the elbow, ankle or shoulder although it is mainly found to occur within the knee. “Your chances of developing bursitis are higher if your job or hobby involves a repetitive movement, for example tennis and golf are common causes of bursitis of the elbow” (http://www.nhs.uk/Conditions/Bursitis/Pages/Introduction.aspx?url=Pages/wh at-is-it.aspx). There are many symptoms of bursitis which includes: Constant pain around the joint Tenderness around the joint Swelling around the joint Difficulty in moving the affected joint Pain becoming worse when moving the affected joint which can also happen during the night In some cases redness around the affected area In some cases the individual may develop a fever The treatment and diagnosis of bursitis includes having a physical examination by a GP in order to see whether or not the individual has bursitis. During the physical examination if the individual has tenderness directly over the bursa, swelling with the bursa and pain with movement of overlying muscles and tendons then it is likely that the individual has bursitis. The individual may then need to have an x-ray in order to confirm the diagnosis. In some cases a MRI scan may be needed, this is usually done if the individual is having difficulty walking. Once an individual knows that they have bursitis then the treatment in which they may be given may be as simple as resting the affected area of the body. The individual may also be recommended to take an anti-inflammatory drug such as ibuprofen in order to reduce the pain and swelling. If the symptoms of bursitis continue after trying the above treatment then they may have to have the bursa drained and have an injection Clare Andrews Page 15 Matt Hopton of a corticosteroid drug which will help to reduce the inflammation. If the individual has an infection then they will have to take a course of antibiotics in order to clear the infection. Task Three – P4 An exercise which involves a ball and socket joint and a hinge joint is football. Football is probably one of the most common types of exercise in which both the ball and socket joint and hinge joint are used. In football the ball and socket joint will be the hip and the hinge joint will be the knee. With the ball and socket joint circular movements can occur and the joints can move in all planes as well as rotation been possible. This therefore means that when the individual kicks the ball in football there hip joint will rotate along with circular movements happening in order for the individual to be able to kick the ball. When the individual kicks the ball abduction will occur as this is when a body part moves to the side or away from the middle. When the individual is moving their leg back towards their body then adduction occurs as this is when a body part moves from the side towards the middle of the body. As the ball and socket joint has a ball which is rounded and which fits in a cavity which is shaped like a cup of another bone, movement is allowed in any direction due to this. With the hinge joint the movement which is available consists of up and down motions which happen in one place. This therefore means that when the individual kicks the ball in football there knee joint will only either go up or down in one motion in order for the individual to be able to kick the ball. When the individual kicks the ball extension will occur as this is when the angle is made larger. When the individual is moving the knee back towards their body then flexion occurs as this is when the joint angle is decreased. As the hinge joint only allows movement which is in a single plane-flexion this then means that movement can only occur in one direction. Clare Andrews Page 16 Matt Hopton Bibliography Apatech. (2006) Bones. [Online] Available at: http://www.apatech.com/patientbone.html (Accessed on 8th January 2008). Biology Online. (2008) Cartilaginous joints. [Online] http://www.biology-online.org/dictionary/Cartilaginous_joint Available at: (Accessed on: Available at: 10th January 2009). Blurt it: society. (2007) Synovial joints. [Online] http://www.blurtit.com/q267341.html (Accessed on: 13th January 2009). Bone Development and Growth. (2008) Bone growth. [Online] Available at: http://training.seer.cancer.gov/module_anatomy/unit3_3_bone_growth.html (Accessed on: 8th January 2008). Family Shock. (2006) Types of synovial joints. [Online] Available at: http://www.shockfamily.net/skeleton/JOINTS.HTML (Accessed on: 11th January 2009). Human bio. (2008) Growth and repair of bones. [Online] Available at: http://katie-humanbio.blogspot.com/2008/04/bone-growth-remodeling-andrepair.html (Accessed on: 8th January 2008). Looking good, feeling good: from the inside out. (2006) Function of a fixed joint. [Online] Available at: http://science.education.nih.gov/supplements/nih6/Bone/guide/info_musculo_ skin-c.htm (Accessed on: 10th January 2009). Medline Plus. (2009) Flat bones. [Online] http://www.nlm.nih.gov/medlineplus/ency/article/002366.htm Available at: (Accessed on: 8th January 2009). Clare Andrews Page 17 Matt Hopton National Osteoporosis Society. (2009) Osteoporosis. [Online] Available at: http://www.nos.org.uk/NetCommunity/Page.aspx?pid=234&srcid=183 (Accessed on: 12th January 2009). National Osteoporosis Society. (2009) Osteoporosis. [Online] Available at: http://www.housingcare.org/downloads/kbase/2207.pdf (Accessed on: 13th January 2009). NHS Choices. (2008) Bursitis. [Online] Available at: http://www.nhs.uk/Conditions/Bursitis/Pages/Introduction.aspx?url=Pages/wh at-is-it.aspx (Accessed on: 14th January 2009). NHS Choices. (2008) Diagnosing Osteoarthritis. [Online] Available at: http://www.nhs.uk/Conditions/Osteoarthritis/Pages/Diagnosis.aspx?url=Pages /what-is-it.aspx (Accessed on: 14th January 2009). Periosteal Reaction. (2007) periosteum within a synovial joint. [Online] Available at: http://www.squidoo.com/periosteum (Accessed on: 12th January 2009). The internet encyclopaedia of science. (2007) Articular capsule. [Online] Available at: http://www.daviddarling.info/encyclopedia/A/articular_capsule.html (Accessed on: 11th January 2009). University of Maryland Medical Centre. (2007) Long Bones. [Online] Available at: http://www.umm.edu/ency/article/002249.htm (Accessed on: 8th January 2009). Wiki Answers. (2008) Fixed joints. [Online] Available at: http://wiki.answers.com/Q/What_is_a_fixed_joint_in_the_skeleton (Accessed on: 9th January 2009). Clare Andrews Page 18 Matt Hopton Zimmer. (2007) Bursitis. [Online] Available at: http://www.zimmer.co.uk/z/ctl/op/global/action/1/id/7999/template/PC/navid/63 3 (Accessed on: 14th January 2009). Clare Andrews Page 19 Matt Hopton