Pancreatitis (W95)
advertisement
")
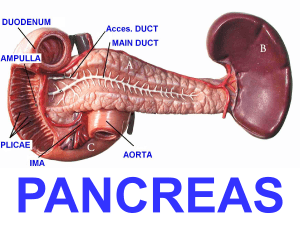
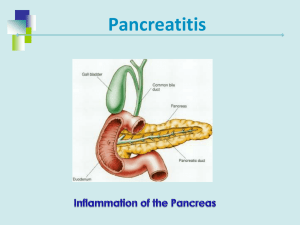
PANCREATITIS Definition: Inflammation of the pancreas Etiology: 1. 2. condition may be either acute or chronic common causes are: a. biliary tract disease (about 1/2 of all patients) b. alcoholism (esp. in chronic disease) c. stomach/biliary tract surgery d. hypolipoproteinemia e. trauma f. viral and bacterial infections (esp. H. pylori, Giardiasis, S. typhi, Streptococcus, Cocksackie) Signs and Symptoms: Acute: 1. severe abdominal pain: a. may radiate to the back, flank, chest, etc. b. it increases over hours and lasts until the inflammation disappears (days to weeks) c. the pain is < supine and > sitting flexed forward with knees up 2. N/V 3. fever of 100-102oF 4. abdominal guarding and rigidity (in 1/3 of patients) 5. occasional rebound tenderness, diminished or absent bowel sounds 6. patient is distressed and anxious 7. tachycardia, hypotension 8. shock may occur 9. Grey Turner's sign or Cullen's sign may appear after a couple of days (ecchymosis on the flanks or around the umbilicus, respectively) 10. Abscesses are common 2-5 weeks after the attack Chronic: 1. upper abdominal pain may be persistent or intermittent a. < after eating, often radiates to the back and is described as aching, gnawing, burning or stabbing b. it typically lasts for days to weeks 2. N/V 3. progression to insufficiency 4. steatorrhea may occur when the pancreas has been severely damaged 5. weight loss 6. abdominal masses may be palpated Lab Findings: Acute: 1. serum amylase concentration begins to rise at 3-6 hours, peaks at 20-30 hours, then declines (> too Somogyi units/ml characteristic) 2. increased: a. urine amylase/creatinine clearance ratio above 5% b. serum TG concentration c. serum lipase remains elevated 14 days after amylase normalizes d. bilirubin may be e. WBCs 3. blood sugar and glycosuria 4. LDH over 700 units, AST/SGOT over 250 S-F units, and/or Pa O2 < 60mmHG indicates a poor prognosis 5. hemoconcentration occurs 6. x-ray of abdomen and chest 7. IV cholangiography 8. US 9. CT scan 10. serum calcium may be decreased 1-9 days after onset (may cause tetany) Chronic: 1. (+) secretin test measuring decreased pancreas exocrine function 2. pancreas x-ray show calcific pancreas (usually in patients with alcoholic history) 3. abdominal US, CT scan, angiography 4. may see increase in serum amylase or lipase (10%) 5. glucose tolerance test mimics diabetic pattern 6. steatorrhea present 1 Jason Schnieder 1998 PANCREATITIS Course/Prognosis: Acute: 1. most patient recover in 5-7 days in cases of mild, uncomplicated acute conditions 2. mortality is about 5% 3. complications include: a. progression to chronicity b. abscesses c. jaundice d. respiratory failure e. acute renal failure 4. the prognosis in acute hemorrhagic or suppurative pancreatitis is very unfavorable, with a mortality rate of 50-90% 5. acute pancreatitis must be treated with utmost urgency to avoid complications 6. acute pancreatitis with LDH over 700 units, AST/SGOT over 250 S-F units, and/or Pa O2 < 60mmHG indicates a poor prognosis Chronic: 1. the pancreatic acinar cells decrease and the patient develops steatorrhea and creatorrhea 2. if islet cell destruction occurs, the patient may develop glucose intolerance and DM 3. the course is gradual and progressive 4. conventional treatment includes the use of pancreatic enzymes, antacids and provision of pain relief Differential Diagnosis: Acute: 1. acute cholelithiasis 2. perforated viscus 3. acute intestinal obstruction 4. mesenteric infarction 5. ectopic pregnancy 6. diabetic coma 7. other causes of acute abdomen Chronic: 1. peptic ulcer 2. gastitis 3. biliary tract disease 4. pancreatic cancer 5. malabsorption 6. Crohn's disease Nutrition: Acute phase: 1. during acute attack nothing is given by mouth, when pain and tenderness ceases use an alkaline fast for 4 days then slowly return to a normal diet a. pancreatin (1.8-2.7g should accompany each meal) 2. fasting/cleansing diet: a. diet should be adequate fiber with low simple carbohydrates, adequate in trace minerals and protein b. chew carbohydrates adequately 3. increase vitamin A, C, D, K, calcium and folic acid foods; vitamin B-12 may be given 1/month 4. increase fluids if Steatorrhea: 1. use low fat diet with medium chain TG (MCT oil) Avoid: 1. 2. 3. 4. 5. 6. 7. heavy protein foods: meat, shellfish hot sauces, spicy, fried, fatty, rich and/or salty foods sweet foods and sugar, white bread dairy products refined and processed foods alcohol, coffee, caffeine catarrh forming foods: tofu, meat, ice cream, shellfish Supplements: 1. vitamin A (50-75,000 IU QD) 2. vitamin B complex 2 Jason Schnieder 1998 PANCREATITIS 3. 4. 5. 6. 7. 8. vitamin B-6 vitamin C (6-8g QD) vitamin E (800 IU QD) magnesium bicarbonate pancreatic enzymes (Aspergillus): wide range of action; SIG: 1-2 at the beginning of meals [will kill Clostridium and other bacteria] 9. papain (papaya): digests protein 10. bromelian (pineapple): digests protein [caustion: can irritate gastric lining, esp. if gastritis is present) Hydrotherapy: 1. constitutional hydrotherapy 2. compress: alternating hot and cold to abdomen (4min./1min.) Manipulation: 1. check and align T5-9 Botanicals: 1. 2. 3. 4. 5. Achillea millefolium: as compress Aconitum napellus (toxic): acute Bryonia alba (toxic) Chionanthus virginica: obstruction of bile ducts due to duodenitis Inula helenium Formulas: a. subacute: Capsicum frutescens, Hydrastis canadensis Homeopathy: 1. Belladonna: congestion; sudden attack; intense pain; constriction of abdomen around the navel as if a fall or lump would form; tenderness of abdomen < least jar, pressure 2. Carbo animalis: indurated pancreas; profuse, tasteless, thin saliva of sweetish, putrid odor; sensation of coldness; apparently rising from the abdomen into throat and mouth; eating causes distress and burning in the stomach; oppression in the epigastrium 3. Conium maculatum: acute pancreatitis; sudden attacks of vomiting and diarrhea at night; vomiting of a white substance containing saliva without any admixture of the contents of either stomach or bowels; trembling of abdomen 4. Iodine: pancreatic disease; severe chill followed by high temp.; swelling, tenderness and cutting pain in abdomen; whitish, whey-like stools; loss of appetite; chronic inflammation; pancreas enlarged; abdominal pulsation's; great thirst; appetite appeased by smallest quantity of food; urine scanty brown, sallow face, depressed, irritable; sensitiveness to pressure; pressure in the region of stomach with much belching; occasionally vomiting of small quantity of tough sour mucus 5. Iris versicolor: vomiting of a sour, bilious, brassy-tasting substance; soreness through the abdomen; stools constipated between attacks but diarrhea during attack; > continued motion; burning distress in region of pancreas; sick h/a periodically every week 6. Kali iodatum: rancid taste in mouth after eating or drinking; viscid satish saliva; burning in pit of stomach; cutting and burning around navel; emaciation and loss of appetite 7. Phosphorus: pancreatic disease; very weak empty sensation in whole abdomen; fatty degeneration; oily stool; stools undigested, containing food particles of fat or looking like cooked sago; pale yellow face anemia; atrophy of pancreas with DM 8. Spongia tosta: chronic pancreatitis; abdomen hard and light 3 Jason Schnieder 1998